
A Rare Occurrence of Metastatic Gastric Adenocarcinoma Causing Acute Spontaneous Tumor Lysis Syndrome and Acute Renal Failure: A Case Report and Review of the Literature
Rohit Venkatesan1*#, Bernard M. Karnath2#, Robert A. Davee2#
Affiliation
- 1Department of Internal Medicine Residency Program, University of Texas Medical Branch
- 2Department of General Internal Medicine, University of Texas Medical Branch
- #Each Author listed contributed sufficiently to the creation of this manuscript
Corresponding Author
Rohit Venkatesan, MD, Department of Internal Medicine Residency Program, University of Texas Medical Branch, 301 University Blvd. John Sealy Annex 4.174 Galveston, TX 77555-0566. Tel: 409.772.4182/ Fax: 409.772.6507; E-mail: rovenkat@utmb.edu
Citation
Venkatesan, R., et al. A Rare Occurrence of Metastatic Gastric Adenocarcinoma Causing Acute Spontaneous Tumor lysis Syndrome and Acute Renal Failure: A Case Report and Review of the Literature. (2015) Int J Cancer Oncol 2(2): 1-4.
Copy rights
© 2015 Venkatesan, R. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Gastroenterology; Oncology; Stomach; Tumor; Case report
Abstract
Tumor lysis syndrome is an oncologic emergency. It is typically seen in malignancies with high tumor burden and is seen much more frequently in hematologic malignancies than in solid tumors. More often, tumor lysis syndrome occurs as a result of anti-cancer treatment, however it can also occur spontaneously. Here we present a rare case, to our knowledge only the third ever reported case, of metastatic gastric adenocarcinoma causing acute spontaneous tumor lysis syndrome.
Introduction
Tumor lysis syndrome (TLS) is an emergent and potentially fatal consequence of anti-cancer treatment. Typically it is seen in malignancies which are rapidly roliferating cancers and/or malignancies with a high tumor burden or high bulk[1-3]. It refers to the lysis of tumor cells which cause a spilling of their cellular contents into the bloodstream. The constellation of signs and symptoms usually include characteristic findings of hyperuricemia, hyperkalemia, hyperphosphatemia, and hypocalcemia. These metabolic disturbances can lead to seizures, cardiac arrhythmias, renal failure and potentially death[1-4].
A rarer phenomenon is spontaneous tumor lysis syndrome (STLS)[5]. This is due to the spontaneous necrosis of tumor cells with spilling of their cellular contents without receiving any anti-cancer treatment. This has been described in hematologic malignancies, but it appears to be an extremely rare occurrence in solid tumors[2,3,6]. An even more uncommon occurrence is for STLS to be caused by a primary tumor consistent with gastric adenocarcinoma[1,2].
Case Presentation
A 60 year-old African American male with a past medical history of coronary artery disease, gastro esophageal reflux disease, and hepatitis C virus infection presented complaining of worsening abdominal pain of four weeks duration. The pain on admission was sharp, cramping, and 10/10 in severity. He denied any aggravating or alleviating factors. The patient described fatigue and a 40 pound weight loss over the past six weeks. He stated that he had been unable to tolerate solid foods over this time. Associated symptoms included shortness of breath, dizziness, and nausea/vomiting. He denied diarrhea or constipation or any signs of gastrointestinal bleeding. The patient reported a 60-pack year smoking history and previous alcohol abuse, drinking 8-12 beers a week currently but states that he used to drink more heavily than this in the past. Physical exam revealed a cachectic male with a firm, tender, distended abdomen and bilateral 2+ lower extremity edema. Profound bilateral axillary and inguinal lymphadenopathy was noted. Laboratory analysis was significant for hyperkalemia with a potassium of 6.4, a creatinine of 3.18 (previous creatinine was 0.81 just two months prior), uric acid of 15.2, calcium of 9.0 and phosphorus of 6.2. The patient was also found to be oliguric. His initial urine output in the first 24 hours of admission was just 320 cc. Nephrology and oncology was consulted at this point as TLS and acute renal failure (ARF) from TLS were suspected. His urine output steadily dropped in the subsequent days despite multiple attempts to force dieresis with furosemide. Creatinine also continued to trend up. One dose of Rasburicase was given which decreased uric acid, and maintenance allopurinol was started. A CT scan of the abdomen and pelvis without contrast revealed marked gastric wall thickening (Figure 1), extensive lymphadenopathy, and moderate ascites with areas of nodularity and hyperdensity suggestive of peritoneal carcinomatosis. A subsequent endoscopy (Figure 2, 3) and gastric biopsy (Figure 4, 5) demonstrated invasive, poorly differentiated gastric adenocarcinoma. A fine needle aspiration of an axillary lymph node and urine cytology both showed high-grade carcinoma consistent with metastasis from a gastric primary tumor (Figure 6, 7). A diagnosis of ARF secondary to acute urate nephropathy was made. The patient was aggressively hydrated for his STLS, but his urine output dropped and his edema and ascites worsened. As he continually failed attempts of forced dieresis, the only option left was hemodialysis. After prognosis was discussed with the patient and family, they decided upon hospice care and to forego hemodialysis.
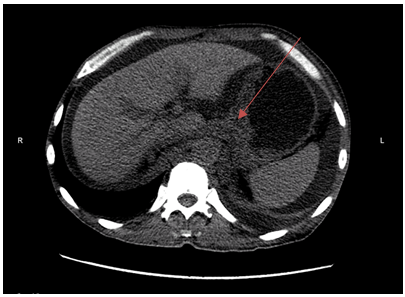
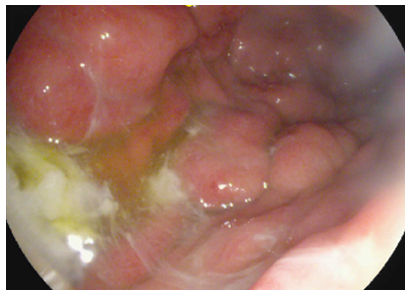
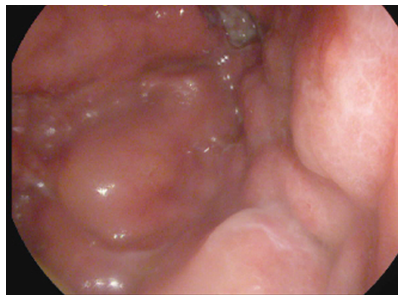
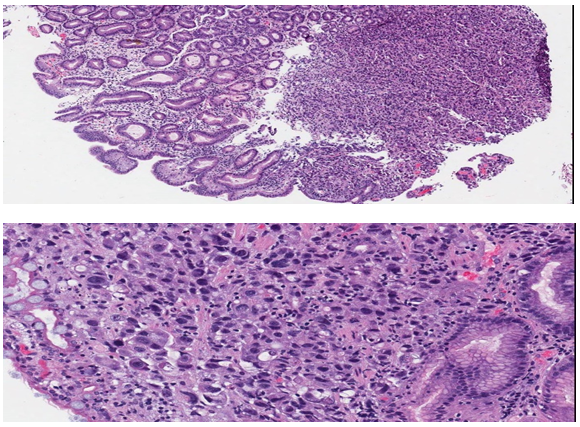
Figure 4 & 5: Gastric adenocarcinoma with infiltrating malignant glands and desmoplastic stromal response.
(Figure 4 and 5 courtesy of Dr. Heather M. Ruff and Dr. Vicki J Schnadig. UTMB department of pathology)
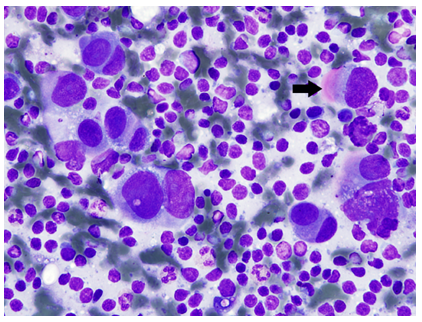
Figure 6: Right axillary lymph node fine needle aspiration. Very large neoplastic cells are seen singly and in small clusters. Shape and distribution of cells are similar to those found in urine (below, Image 7) and are compatible with metastasis from poorly differentiated gastric carcinoma. (Romanowski stain).
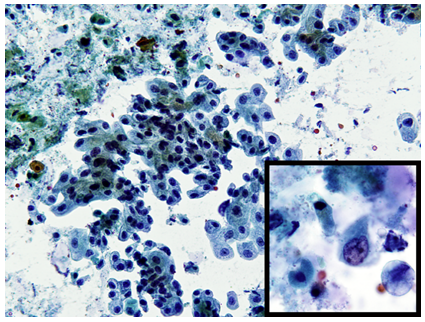
Figure 7: Urine, catheterized. Abundant neoplastic cells are seen in loosely cohesive sheets and singly. Cells have moderate amounts of foamy cytoplasm and central to eccentric nuclei with irregular nuclear membranes. Shape and distribution are compatible with metastasis from poorly differentiated gastric carcinoma. (Papanicolaou stain).
(Figures 6 and 7 courtesy of Dr. Vicki J Schnadig. UTMB department of pathology)
Discussion
As previously mentioned, TLS and STLS are oncologic emergencies and potentially fatal conditions due to the aforementioned causes of cardiac arrhythmia, seizures or acute renal failure (ARF)[1-4]. In our case, our patient eventually developed acute urate nephropathy causing ARF. Recent literature has indicated that in-hospital and 6 month mortality rates were much higher for patients who experienced TLS causing ARF than for patients with TLS not experiencing ARF. Mortality rates for patients experiencing ARF ranged anywhere from 51-66% as compared to 7-21% for patients not experiencing ARF[7]. Older literature has described the mortality rate for acute urate nephropathy to be as high as 47-100%[8,9].
Though rare, when it does occur TLS and STLS are usually seen in cancers with high cellular turnover and high tumor burden[1-3]. In earlier literature, it was more thoroughly described in lymphomas and leukemias[4-10] and though in recent literature it has been described in several different solid tumor types, it remains an exceedingly rare occurrence in solid tumors[1-3,11]. There are approximately only 100 cases of TLS and STLS described in the literature for patients with solid tumors since 1977[3]. The majority of these cases were chemotherapy induced, indicating non-spontaneous TLS, meaning that STLS with solid tumors remains exceedingly rare[3,5]. All reported cases of STLS and TLS in solid tumors involved patients who had a high tumor burden. Metastatic disease was present in 83% of these cases and a bulky primary tumor (>10 cm) was present in 17% of the cases[3]. Gastric adenocarcinoma as a primary tumor type causing STLS appears to be an exceedingly rare cause of this phenomenon. The first case was described in 2001[2] and the most recent case described in 2014[1]. To our knowledge these are the only cases reported of STLS with a gastric denocarcinoma primary tumor. STLS in solid tumors as a cause for ARF as was the case in our patient is also an extremely rare occurrence[6,12], and in our case was the primary reason for an increase in morbidity and mortality.
Although we have emphasized the rarity of cases of TLS and STLS in solid tumors, their reported incidence has increased somewhat in recent years[1,4,5]. As cases of TLS and STLS continue to be recognized, described and reported it is of paramount importance to recognize the possibility of their occurrence in patients with solid tumors. It has been described that the mortality rate for TLS in solid tumors is higher when compared to its occurrence in hematologic malignancies[13,14]. Despite the incidence being much higher in hematologic malignancies[11,13], it was found that TLS in solid tumors had a mortality rate of greater than one in three[13,14] compared to at most 13% in hematologic malignancies[15]. Further work has demonstrated that undiagnosed or late-diagnosed TLS in solid tumors can increase mortality rate by 20-50%[6]. It remains unclear whether the syndrome itself is more aggressive with solid tumors, or these statistics reflect a lack of prophylactic measures and/or awareness against TLS in solid tumors[14].
Conclusion
In conclusion, we present our case for several different reasons. The first is to report an exceedingly rare case of STLS with a gastric adenocarcinoma primary tumor. To our knowledge, this is only the third reported case of such an occurrence[1,2]. Moreover, however, we emphasize that TLS and STLS are oncologic emergencies that are potentially fatal and must be recognized promptly to avoid life-threatening consequences[1-4]. In recent literature, there are more cases being described of TLS and STLS in solid tumors, though it remains a very rare occurrence[2-6]. Interestingly, there is further evidence emerging that these entities may be under-recognized in solid tumors and may be more prevalent than initially thought[5]. With the mortality and morbidity associated with this condition and associated ARF[7] prompt recognition is vital and a higher index of suspicion for this syndrome in patients with solid tumors, regardless of the initiation of anti-cancer treatment, may certainly be warranted based on our case and other recent literature.
Acknowledgement: Dr. Heather, M., Ruff, D.O., Dr. Vicki, J. Schnadig, MD. The University of Texas Medical Branch Department of Pathology
Financial Support: No Financial support was provided to any of the authors for the creation/writing of this manuscript
Conflicts of Interest: There are NO potential conflicts of interests with any of the authors on the creation/writing of this manuscript
Informed Consent: Informed consent was obtained from all involved patients. All identifying information has been removed in the manuscript
References
- 1. Goyal, H., Sawhney, H., Bekara, S., et al. Spontaneous acute tumour lysis syndrome in gastric adenocarcinoma: a case report and literature review. (2014) J Gastrointest Cancer 45 Suppl 1: 208- 211.
- 2. Woo, I.S., Kim, J.S., Park, M.J., et al. Spontaneous acute tumor lysis syndrome with advanced gastric cancer. (2001) J Korean Med Sci 16(1): 115- 118.
- 3. Vodopivec, D.M., Rubio, J.E., Fornoni, A., et al. An unusual presentation of tumor lysis syndrome in a patient with advanced gastric adenocarcinoma: case report and literature review. (2012) Case Rep Med 2012: 468452.
- 4. Howard, S.C., Jones, D.P., Pui, C.H. The tumor lysis syndrome. (2011) N Engl J Med 364(19): 1844- 1854.
- 5. Vaisban, E., Braester, A., Mosenzon, O., et al. Spontaneous tumor lysis syndrome in solid tumors: really a rare condition? (2003) Am J Med Sci 325(1): 38- 40.
- 6. Coiffier, B. Acute tumor lysis syndrome - a rare complication in the treatment of solid tumors. (2010) Onkologie 33(10): 498- 499.
- 7. Darmon, M., Guichard, I., Vincent, F., et al. Prognostic significance of acute renal injury in acute tumor lysis syndrome. (2010) Leuk Lymphoma 51(2): 221- 227.
- 8. Garnick, M.B., Mayer, R.J. Acute renal failure associated with neoplastic disease and its treatment. (1978) Semin Oncol 5(2): 155- 165.
- 9. Kjellstrand, C.M., Cambell, D.C., von Hartitzsch, B., et al. Hyperuricemic acute renal failure. (1974) Arch Intern Med 133(3): 349- 359.
- 10. Hsu, H.H., Huang, C.C. Acute spontaneous tumor lysis in anaplastic large T-cell lymphoma presenting with hyperuricemic acute renal failure. (2004) Int J Hematol 79(1): 48- 51.
- 11. Kekre, N., Djordjevic, B., Touchie, C. Spontaneous tumour lysis syndrome. (2012) CMAJ 184(8): 913- 916.
- 12. Agnani, S., Gupta, R., Atray, N.K., et al. Marked hyperuricemia with acute renal failure: need to consider occult malignancy and spontaneous tumour lysis syndrome. (2006) Int J Clin Pract 60(3): 364- 366.
- 13. Baeksgaard, L., Sørensen, J.B. Acute tumor lysis syndrome in solid tumors--a case report and review of the literature. (2003) Cancer Chemother Pharmacol 51(3): 187- 192.
- 14. Kalemkerian, G.P., Darwish, B., Varterasian, M.L. Tumor lysis syndrome in small cell carcinoma and other solid tumors. (1997) Am J Med 103(5): 363- 367.
- 15. Coiffier, B., Altman, A., Pui, C.H., et al. Guidelines for the management of pediatric and adult tumor lysis syndrome: an evidence-based review. (2008) J Clin Oncol 26(16): 2767- 2778.










