
B-Cell Lymphoma, Unclassifiable, with Features Intermediate between Diffuse Large B-Cell Lymphoma and Classical Hodgkin Lymphoma: A Review of Reported Cases
Omar Nadeem1*, Jorge J. Castillo2, Diana O.Treaba1, James N. Butera1
Affiliation
- 1Pharmacology Department; College of Medicine and Health Sciences-UAE University, UAE
- 2Senior Pharmacist, Tawam Hospital, Abu Dhabi Health Services-UAE
Corresponding Author
Omar Nadeem, Brown University, Rhode Island Hospital, 593 Eddy St, Providence, RI 02903, USA, Tel: 401444.5435 ; Fax: 401.444.5256 ; E-mail: onadeem@lifespan.org
Citation
Nadeem, O., et al. B-Cell Lymphoma, Unclassifiable, with Features Intermediate between Diffuse Large B-Cell Lymphoma and Classical Hodgkin Lymphoma: A Review of Reported Cases. (2014) J Cancer Oncol 1(1): 1-4.
.
Copy rights
© 2014 Nadeem, O. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Grey zone; Unclassifiable; Lymphoma
Abstract
Grey Zone Lymphoma (GZL), with features intermediate between classical Hodgkin lymphoma (cHL) and diffuse large B-cell lymphoma (DLBCL), is a new entity with limited reported data. A MEDLINE search through July 2013 identified 39 cases of GZL and two additional cases were added from our institution. Comparison of complete remission (CR) rates between ABVD and CHOP-based regimens was performed using Fisher’s exact test. The median age of presentation was 33.5 years with a male predominance (59%), mediastinal involvement (89%), and early stage disease (75%). Patients treated with CHOP-based regimens achieved higher CR rates compared to initial ABVD-based regimens (80% vs. 0%;p=0.01). The 2-yr OS was 87% with a median OS that was not reached. Our reviewindicates this lymphoma subtype to have a high incidence of early stage presentation, mediastinal involvement, B symptoms and overall better outcomes with CHOP-based regimens. Additional studies are warranted to further study this disease.
Introduction
Non - Hodgkin lymphomas (NHL) are a group of clonal lymphoid neoplasms that arise from either progenitor or mature B- or T - cells. In the United States, NHL is the fifth most common malignancy and the sixth most common cause of cancer - related death[1]. B - cell lymphomas account for the majority of NHL cases worldwide, and diffuse large B - cell lymphoma (DLBCL) is the most common histological subtype, accounting for roughly 25% of cases[2,3]. It has become increasingly apparent that DLBCL is a heterogeneous group with variable clinical and biological behavior and recent efforts have been made to further sub - classify this entity[4, 5].
World Health Organization (WHO) classification of Tumors of the Hematopoietic and Lymphoid Tissues serves as the gold standard for categorization of various hematological malignancies and uses clinical information, morphology, cytogenetics and immuno phenotyping for further sub-classification. In 2008, the WHO proposed new entities to further sub - classify lymphomas with overlapping features. These are termed B-cell lymphoma, unclassifiable with features intermediate between "DLBCL and either classical Hodgkin lymphoma (cHL) or Burkitt lymphoma (BL)[3]. These entities were not clearly classified previously in the literature, being designated as "Grey Zone Lymphomas (GZL)" making conclusions about their clinical behavior and best management strategy difficult. The B - cell lymphoma, unclassifiable with features intermediate between DLBCL and cHL, raises challenging treatment considerations. DLBCL is treated with combination chemo immunotherapy usually consisting of cyclophosphomide, doxorubicin, vincristine and prednisone (CHOP), along with anti - CD20 monoclonal antibody rituximab[6]. Treatment for cHL generally requires a different combination chemotherapy regimen, which most commonly includes doxorubicin, bleomycin, vinblastine and dacarbazine (ABVD), with or without radiation therapy depending on disease stage[7, 8]. With the newly proposed entity of B-cell lymphoma, unclassifiable with features intermediate between DLBCL and cHL, no current consensus exists in terms of the optimal management strategy. We aimed to review the literature of all reported cases of this entity to better define its presenting clinical characteristics, outcome to therapy and prognosis.
Materials and Methods
A comprehensive MEDLINE search was performed through July 2013 using key words "gray zone" or "unclassifiable or indeterminate" and "lymphoma". Cases were included in the analysis if they met the pathological definition of B - cell lymphoma, unclassifiable with features intermediate between DLBCL and cHL as defined by the WHO criteria, based on morphological and immunophenotypic pattern. Cases without primary pathological immunophenotypic information or primary clinical patient data were excluded.
Our search yielded a total of 554 abstracts. All abstracts were reviewed to determine relevancy and 45 articles met study criteria for additional comprehensive review to identify individual cases. From these, a total of 39 unique cases were identified from 8 articles[9-16], along with two additional cases from our local institution, for total number of cases of 41. Strict pathological eligibility criteria was implemented, using morphological and immunophenotypic data, and pathological review of the reported immuno histochemical pattern was conducted by our staff hematopathologist(DOT) to insure compatibility with a diagnosis of GZL per the WHO criteria.
Baseline demographic data were collected along with clinical presentation, stage, and pathological data including morphology, immunophenotype pattern and EBV status. Treatment data, if available, were also collected and comparison of complete remission (CR) rates between ABVD and CHOP-based regimens were performed using Fisher's exact test[17]. P values of <0.05 were considered statistically significant. Overall survival (OS) was defined as the time elapsed between lymphoma diagnosis and death or last follow-up, and was estimated using the Kaplan - Meier method[18].Statistical analysis was performed using MedCalc Statistical Software version 13.1.0 (MedCalc Software bvba, Ostend, Belgium, 2014).
Results
Patient demographic data are presented in Table 1. The median age of presentation was 33.5 years (range 13 - 85 years) with a slight male predominance (59%). Clinical data were available for review for 20 of the 41 patients. B symptoms were present in 77% of cases and 75% presented with an early stage (I or II). Mediastinal lymphadenopathy was the most common site of disease and was present in 89% of cases. Pathological data was noted for a majority (68%) of patients having a morphological appearance of cHL with Reed-Sternberg cells. Immunophenotype pattern revealed a high rate of CD20 (90%) and CD30 (95%) positivity while only 63% were CD15 positive (Table 1). Of the 22 patients who were assessed for EBV status based on EBER and/or LMP1 expression, 9 (41%) were positive.
Table 1: Baseline Characteristics
| Age (years) | 33.5(range 13-85) |
|---|---|
| Sex Male | 59% |
| Female | 41% |
| Early stage (I or II) | 75% |
| B symptoms | 77% |
| Mediastinal Involvement | 89% |
| Morphology | Reed Sternberg cells (68%) |
| EBV positive | 41% |
| Immunophenotype | |
| CD20 | 90% |
| CD30 | 95% |
| CD15 | 63% |
| CD45 | 73% |
| CD79a | 100% |
| PAX5 | 100% |
| OCT2 | 72% |
Table 2: Treatment Outcomes
| PR | CR | ORR | P value | |
|---|---|---|---|---|
| CHOP-like (n=5) | 1 | 4 | 100% | 0.05 |
| ABVD (n=7) | 3 | 0 | 43% |
Treatment pattern is summarized in Table 2. Patients were either treated with initial cHL regimens (BEACOPP, ABVD) or DLBCL regimens (CHOP, EPOCH, with or without rituximab). Seven patients received initial treatment with ABVD-based regimens, of which four (57%) did not respond and three (43%) achieved a partial response (PR). There were no reported CRs. Of the seven patients treated with CHOP-based regimens, five had clinical outcome data available. Four patients (80%) achieved a CR and one (20%) achieved a PR (Fisher's for CR rate P=0.01). All patients that achieved CR after CHOP-based regimens received consolidation radiation therapy. Seven patients underwent an autologous stem cell transplantation, of which there were two reported relapses within the first 6 months. Survival data were available in 15 (37%) patients. The median follow-up for the entire cohort was 15 months and the 2 - yr OS was 87% with a median OS that was not reached (Figure 1).
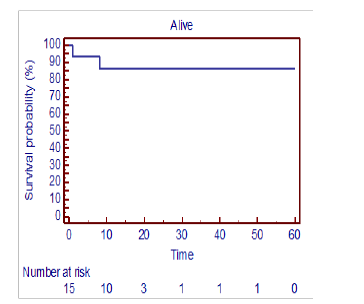
Figure 1: Kaplan-Meier Overall survival (OS) estimate for 15 patients with Grey Zone Lymphoma (GZL)- B-cell lymphoma, unclassifiable with features intermediate between classical Hodgkin Lymphoma (cHL) and Diffuse Large B-cell Lymphoma (DLBCL) treated with chemotherapy.
Discussion
B - cell lymphoma, unclassifiable with features intermediate between DLBCL and cHL, is a relatively new entity per the latest WHO classification. Due to its rarity, there is little reported on clinical data, therapy and outcomes. We performed a comprehensive literature review to identify individual cases to better understand the clinical characteristics and natur-al history of this rare lymphoma subtype.Our results reveal several important points. First, it appears that the majority of patients with this entity present with early stages, mediastinal involvement and B symptoms. Therefore, one's suspicion for this rare entity should be heightened when encountering a patient with the classic immunophenotype of this GZL and these presenting clinical characteristics.
Second, it appears that treatment of this entity with CHOP-like regimens appear to have better outcomes as the reported CR rates are higher than with ABVD - based regimens. Given the proclivity of this lymphoma to involve the mediastinum and its poor response to cHL regimens, one can speculate that many of these patients may have been previously inappropriately classified as refractory cHL Nonetheless, it is of interest that outcomes for these patients seem to be improved with CHOP - like regimens as opposed to ABVD - based regimens. Although, the numbers of patients analyzed in this study for treatment response were small and the conclusion might be spurious, this result remained statistically significant and is a novel finding worth of further investigation.
Of note, all patients who achieved a CR after CHOP - like regimens were consolidated with radiation therapy, which may be important in the management of this disease. However, the role of radiation therapy in this disorder will have to be further defined in larger studies.
The role of rituximab in this disease is intriguing and deserves further study as most of these lymphomas are CD20 positive. However, rituximab use was not universal and was used in less than half (3/7) of the patients treated with CHOP-like regimens. Therefore, from this data set it is not possible to make conclusions on the benefit of rituximab in this lymphoma subtype. Furthermore, it is unclear if the addition of rituximab to ABVD - based regimens would improve disease outcomes. Also, it is noteworthy that this review revealed that this rare lymphoma subtype is almost always CD30 positive, lending to the possible role of brentuxima bvedotin in future study of these patients. Lastly, the rate of EBV positivity was high in our analysis. EBV positivity is seen in 20 - 50% of cHL in North American and European reports[19]. EBV has also been reported infrequently in DLBCL although with higher rates in immuno compromised patients and in the elderly[20]. The finding of EBV positivity in this GZL subtype has been reported by other authors[10]; however, the high incidence EBV positivity in this analysis adds evidence that this GZL could be included onto a growing list of EBV - associated lymphomas. However, the implications of this association are unclear at this point.
Our study has several limitations. First, while the retrospective nature of this study allows for better disease characterization and comprehension, it does limit widespread conclusions regarding treatment outcomes. Second, despite a comprehensive literature search, the number of reported cases was small, possibly indicating the rarity of this newly defined disease entity. Lastly, due to the literature review nature of this study, no central review of pathology was undertaken which also is a limitation of this analysis. However, given the rarity of this entity, large trials with central pathology reviews may be challenging to perform.
Conclusion
B-cell lymphoma, unclassifiable with features intermediate between DLBCL and cHL, is an evolving entity with limited clinical data. Our study reveals a high incidence of early stage presentation, mediastinal involvement, B symptoms and EBV positivity. CHOP - like regimens appear to have more favorable outcomes when compared to ABVD - based regimens. Prognosis of this rare lymphoma subtype, however, appears favorable. Future larger studies are needed to validate these results.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
- 1. Surveillance, Epidemiology, and End Results Program (SEER). (2011) Database (internet).
- 2. Campo, E., Swerdlow, S.H., Harris, N.L., et, al. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. (2011) Blood 117(19): 5019- 5032.
- 3. Morton, L.M., Wang, S.S., Devesa, S.S., et al. Lymphoma incidence patterns by WHO subtype in the United States, 1992-2001. (2006) Blood 107(1): 265- 276.
- 4. Alizadeh, A.A., Eisen, M.B., Davis, R.E., et al. Distinct types of diffuse large B - cell lymphoma identified by gene expression profiling. (2000) Nature 403(6769): 503- 511.
- 5. Rosenwald, A., Wright, G., Chan, W.C., et al. The use of molecular profiling to predict survival after chemotherapy for diffuse large-B-cell lymphoma. (2002) N Engl J Med 346(25): 1937- 1947.
- 6. Coiffier, B., Lepage, E., Briere, J., et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. (2002) N Engl J Med 346(4): 235- 242.
- 7. Fermé, C., Eghbali, H., Meerwaldt, J.H., et al. Chemotherapy plus involved-field radiation in early-stage Hodgkin's disease. (2007) N Engl J Med 357(19): 1916- 1927.
- 8. Canellos, G.P., Anderson, J.R., Propert, K.J., et al. Chemotherapy of advanced Hodgkin's disease with MOPP, ABVD, or MOPP alternating with ABVD. (1992) N Engl J Med 327(21): 1478- 1484.
- 9. Cogen, A., Bries, G., Verbeke, S., et al. Unclassifiable B - cell lymphoma occurring after necrotizing pneumonia. (2013) Eur J Cardiothorac Surg 43(3): e89- e91.
- 10. Wang, E., Papavassiliou, P., Sebastian, S. A malignant lymphoma with histological features and immunophenotypic profile intermediate between EBV-positive diffuse large B-cell lymphoma and EBV-positive classical Hodgkin lymphoma in a 67-year-old female: a "gray zone" lymphoma associated with Epstein-Barr virus in the elderly. (2012) Pathol Res Pract 208(6): 363- 367.
- 11. Gualco, G., Natkunam, Y., Bacchi, C.E. The spectrum of B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma: a description of 10 cases. (2012) Mod Pathol 25(5): 661- 674.
- 12. Minami, J., Dobashi, N., Asai, O., et al. Two cases of mediastinal gray zone lymphoma. (2010) J Clin Exp Hematop 50(2): 143- 149.
- 13. Traverse - Glehen, A., Pittaluga, S., Gaulard, P., et al. Mediastinal gray zone lymphoma: the missing link between classic Hodgkin's lymphoma and mediastinal large B-cell lymphoma. (2005) Am J Surg Pathol 29(11): 1411- 1421.
- 14. Liang, X., Greffe, B., Cook, B., et al. Gray Zone Lymphomas in Pediatric Patients. (2011) Pediatr Dev Pathol 14(1): 57- 63.
- 15. Lynnhtun, K., Varikatt, W., Pathmanathan, N. B Cell lymphoma, unclassifiable, with features intermediate between diffuse large B cell lymphoma and classical Hodgkin lymphoma: Diagnosis by fine-needle aspiration cytology. (2013) Diagn Cytopathol 42(8): 690- 693.
- 16. Iwaki, N., Sato, Y., Kurokawa, T., et al. B-Cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma without mediastinal disease: mimicking nodular sclerosis classical Hodgkin lymphoma. (2013) Med Mol Morphol 46(3): 172- 176.
- 17. Thomas, R.G., Conlon, M. Sample size determination based on Fisher’s Exact Test for use in 2 x 2 comparative trials with low event rates. (1992) Control Clin Trials 13(2): 134- 147.
- 18. Bland, J.M., Altman, D.G. Survival probabilities (the Kaplan-Meier method). (1998) BMJ 317(7172): 1572.
- 19. Chetaille, B., Bertucci, F., Finetti, P., et al. Molecular profiling of classical Hodgkin lymphoma tissues uncovers variations in the tumor microenvironment and correlations with EBV infection and outcome. (2009) Blood 113(12): 2765- 3775.
- 20. Castillo, J.J., Beltran, B.E., Miranda, R.N., et al. Epstein-barr virus-positive diffuse large B-cell lymphoma of the elderly: what we know so far. (2011) Oncologist 16(1): 87- 96.










