
Case Report: Carcinoma of Colon.
Adham Darweesh
Affiliation
1 Consultant Radiologist, Clinical Imaging Department, Hamad Medical Corporation, HGH, Doha, Qatar, Assistant Professor in Clinical Radiology, Weil Cornel Medical College, Qatar (WCMC-Q)
2 Senior Consultant Radiologist, Clinical Imaging Department, Hamad Medical Corporation, HGH, Doha, Qatar, Assistant Professor in Clinical Radiology, Weil Cornel Medical College, Qatar (WCMC-Q)
Corresponding Author
Sushila Ladumor, Consultant Radiologist, Clinical Imaging Department, Hamad Medical Corporation, HGH, Doha, Qatar, Assistant Professor in Clinical Radiology, Weil Cornel Medical College, Qatar (WCMC-Q) E-mail: drsbladumor@yahoo.com
Citation
Sushila, L. Carcinoma of Colon (2018) J Gastrointest Disord Liver Func 4(1): 1- 3.
Copy rights
© 2018 Doria, E. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Colorectal carcinoma (CRC); CT Scan; MRI; Early detection; Colonoscopy; Gastro-Intestinal (GI); Barium enema
Abstract
Colorectal cancer is a disease that is curable if diagnosed at early stage and also it is preventable if predisposing adenomas are detected and removed. Colorectal Carcinoma (CRC) is commonest malignancy of the gastrointestinal tract and is the second most usually diagnosed cancer in adults, mainly at 6th to 7th decades of life[2]. CT and MRI are the modalities of choice used for staging. Colonoscopy for better evaluation and tissue diagnosis as well as to see other occult lesion. Surgical resection may be curative although five-year survival rate is 40 - 50 %.
Introduction
Clinical History 57 year old male patient presented with altered bowel habit, abdominal pain and distension.
Work-up
Figure 1: X-ray Abdomen supine projection
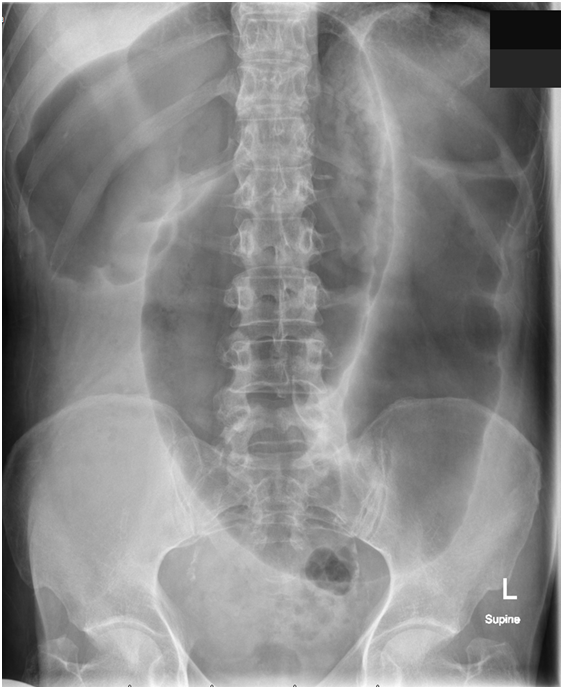
Figure 1: X-ray Abdomen supine projection: Dilated air filled right and transverse colon with non-distended rectum showing some air and fecal material indicating left colon obstruction. No dilated air filled small bowel. No obvious bony lesion.
Figure 2 & 3: CT Scan of Abdomen and Pelvis recommended and done with oral and IV contrast:
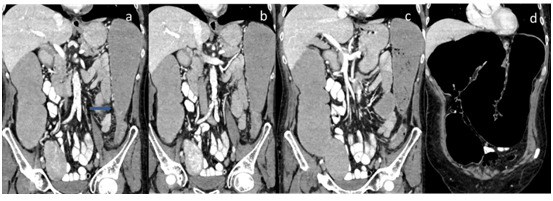
Figure 2: Coronal reconstruction of contrast enhanced CT scan reveal dilated colon up to distal left colon with transitional zone (sown by arrow in image a). Minimal fat stranding noted. No enlarge regional, abdominal or retroperitoneal lymph nodes. Atheromatous vascular changes noted.
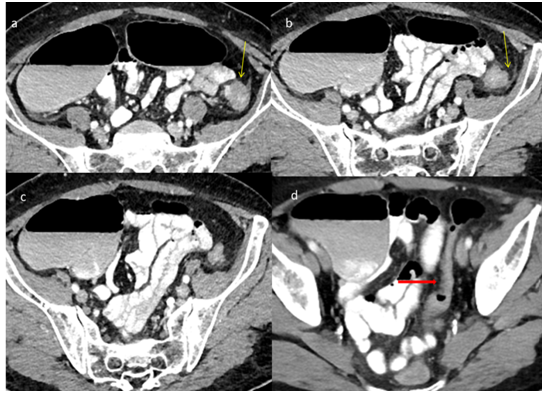
Figure 3: Axial images of contrast enhanced CT scan reveal dilated colon up to distal left colon with transitional zone (sown by yellow arrow in image a & b). It shows irregular outline and slight heterogeneous enhancement and minimal fat stranding noted. No enlarge regional, abdominal or retroperitoneal lymph nodes. Sigmoid and rectum is not dilated (shown by red arrow in image d).
No liver or lung metastases. (Images not shown)
Colonoscopy Reveals narrowing and thickening at distal left colon of about 4 cm segment. Biopsy revealed Adenocarcinoma of colon.
Discussion
Colorectal cancer is the second most common cause of cancer death in developed countries[1]. In 1998, there were 131,000 new cases of colorectal cancer and 56,000 deaths in the United States[2]. In 2014, there were an estimated 1.3 million people with colorectal cancer in the United States. It is estimated that in 2017, there will be 135,430 new cases diagnosed in the United States and an estimated 50,260 people will die of the disease. According to the NIH SEER program, rates of colorectal cancer have been declining approximately 2.7% each year over the past 10 years, with death rates declining by 2.5% each year (2005 - 2014)[3].
Colorectal carcinoma is common; accounting for 15% of all newly diagnosed cancers, and tends to be a disease of the elderly, with the median age of diagnosis between 60 and 80 years of age, slightly younger for rectal carcinoma.
Clinical presentation is typically sneaking, with altered bowel habit or iron deficiency anemia from chronic occult blood loss. Patient can present with symptoms of bowel obstruction, intussusception, heavy bleeding and metastatic disease. Sometime it is detected incidentally by CT done for other reason[1].
Previously Colonoscopy or double contrast (air-barium) enema was used to diagnosed colorectal carcinoma; however, recently widely available Computed Tomography (CT) becomes initial imaging modality of choice in patients with a variety of gastrointestinal symptoms and suspected GI malignancy. Generous use of CT for evaluation of GI pathology the radiologist may be the first to suggest the diagnosis of colon cancer on the basis of CT findings as in this case. Many times colon cancer detected or suspected on colonoscopy and CT or MRI recommended for better evaluation and staging to plan treatment and for follow-up[2]. Continued advancements in scanner and computer technology with CT colonography to play a major role in detection of polyps and early-stage colon cancer in a comfortable way as many patients cannot tolerate or like colonoscopy.
Approximately 30 % of colorectal cancers occur in the sigmoid, 25% occur in the rectum, and 25% occur in the cecum and ascending colon. The remaining 20% of cancers occur in the transverse and descending colon[1,3].
MRI is very useful for local staging of rectal and anal canal tumor as well as in follow-up.MRI has a staging accuracy of and sensitivity for lymph node metastases. MR is having an increasing role to play in the staging of rectal cancer.
Sonography, CT, and MR imaging also play a role in identifying sites of distant metastatic disease, mainly in the liver because limited disease spread to the liver can be surgically resected for cure. Transabdominal sonography is the least sensitive of the three modalities. Although intraoperative sonography obviously cannot be used for screening, this technique is considered the most sensitive means of detecting liver lesions, with a reported sensitivity of at least 95% and it is used now days in operation theatre to evaluate occult lesion that is not seen by other modality as well as for planning of surgical removal.
Once a tumor is invasive, it can extend through the layers of the colonic wall and invade adjacent structures. Lymphatic, hematogenous, and peritoneal spread may also occur. The overall prognosis and outcome depend on the stage of the tumor at diagnosis.
Staging:
The TNM classification system, established by the Union International Contre Le Cancer[3]
| Classification | Definition of TNM Classification |
|---|---|
| Primary tumor (T) | |
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| Tis | Carcinoma in situ |
| T1 | Tumor invades submucosa |
| T2 | Tumor invades muscularispropria |
| T3 | Tumor invades through muscularispropria into subserosa or into nonperitonealizedpericolic or perirectal tissues |
| T4 | Tumor perforates the visceral peritoneum or invades adjacent organs or structures |
| Lymph nodes (N) | |
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Metastasis in from one to three regional lymph nodes |
| N2 | Metastasis in more than four regional lymph nodes |
| Distant metastasis (M) | |
| MX | Presence of distant metastasis cannot be assessed |
| M0 | No distant metastasis |
| M1 | Distant metastasis |
Lists the stage that corresponds to the combined TNM classification and the modified Dukes’ classification.
| Staging of Colorectal Cancer Based on Classifications Using Two Systems | ||||
| Stage of Colorectal Cancer | Classification System | |||
| TNM | Modified Dukes' | |||
| T | N | M | ||
| 0 | Tis | N0 | M0 | |
| I | T1, T2 | N0 | M0 | A (Penetration into but not through the bowel wall) |
| II | T3, T4 | N0 | M0 | B (Penetration through the bowel wall) |
| III | Any T | N1, N2 | M0 | C (Lymph node involvement regardless of extent of bowel wall penetration) |
| IV | Any T | Any N | M1 | D (Distant metastases present) |
Treatment and prognosis
Treatment involves local control with resection in almost all cases. Adjuvant chemotherapy is reserved for stage III disease. Overall 5 year survival rate is 40 - 50%, with stage at operation the single most important factor affecting prognosis. In case of late presentation with acute obstruction or obstruction with perforation immediate surgery or intervention performed to relieve symptoms. For this patient treatment plan was resection and patient travel to home country for surgery.
Teaching point: Whenever patient present with pain and constipation or other relevant GI symptoms and X-ray shows dilated segment of colon with distal non-dilated colon an in adult patient colonic malignancy should be suspected and CT is recommended for better evaluation. Sometimes patient present late with obstructive colonic symptoms when Ileocecal junction is incompetent and we see dilated small bowel as well as colon.
References
1. Horton, K.M., Abrams, R.A., Fishman, E.K. Spiral CT of Colon Cancer: Imaging Features and Role in Management. (2000) radiographics20(2): 419-430.
2. Caroline, R.T. Colon Cancer Imaging. (2017).
Pubmed||Crossref||Others
3. Iyer, R.B., Silverman, P.M. et al. Imaging in the Diagnosis, Staging, and Follow-Up of Colorectal Cancer. (2002) AJR Am J Roentgenol 179(1): 3-13.










