
Dental implants displaced into the mandibular corpus: clinical note.
Felice Lorusso2, Pablo Santos de Oliveira3, Giovanna Murmura45
Affiliation
1 Department of Medical, Oral and Biotechnological Sciences and Cesi-Met University “G. D’Annunzio” of Chieti-Pescara, Italy
2 Department of Oral Surgery, Dental School, University of Chieti-Pescara
3 Department of Oral Implantology, Dental Research Division, College Ingà, UNINGÁ, Cachoeiro de Itapemirim, ES, Brazil
4 Professor, Department of Periodontology, Albanian University and private practice, Tirana, Albania
5 Chief of Maxillofacial Surgery, University of Ferrara, Italy
Corresponding Author
Antonio Scarano, MD, DDS, Dept. of Medical, Oral and Biotechnological Sciences, University “G. D’Annunzio”, Via dei Vestini 31, 66100 Chieti (CH), Italy, Tel: 0871-3554084; Fax: 0871-3554373; E-mail: ascarano@unich.it
Citation
VScarano, A., et al. Dental Implants Displaced into the Mandibular Corpus: Clinical Note. (2018) J Dent Oral Care 4(1): 8- 12.
Copy rights
© 2018 Scarano, A . This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Dental implant complication, Dental implants displaced, Trabecular bone
Abstract
Purpose: Implant migration into the mandibular corpus is a complication reported few times in literature. The aim of study was to describe the clinical characteristics of patients who developed implant displacement into the mandibular corpus, to identify potential risk factors, and to gather information on prevention and treatment of this complication.
Methods: We report three cases of implants displaced into the mandibular corpus laterally of mental nerve. Two implants were removed by screwdriver, in only one case an osteotomy was performed with a Piezosurgery device and it was removed with pliers.
Results: All patients treated had a trabecular bone not observable with a panoramic radiograph, but they showed in the CBCTs performed after implant migration. In these cases, there is no inflammation or pain, but it is necessary to remove the implant and replace a new implant. None of them had a medical history of osteoporosis.
Conclusions: The displacement of implants in the mandibular corpus is not a serious complication, but they must be removed as soon as possible, as the bone healing makes it difficult to remove them later.
Introduction
Placement of implants in the mandible, either with or without ridge augmentation with autogenous bone grafts or bone substitutes, is a generally accepted procedure with a reasonably good prognosis and few complications. Insufficiency of bone tissue represents one of the most frequent problems in implant prosthetic rehabilitation in the posterior mandible[1-3]. In this situation there is a rather high inherent risk of displacement of the implant onto the inferior alveolar nerve which can cause serious ongoing complications. Mandible atrophy also makes it more susceptible to invasion of the inferior alveolar nerve (IAN) during implant site preparation and during implant placement[4].
Nonetheless, nowadays implant rehabilitation of patients has become a quite predictable procedure. Many of the complications can be resolved without severe problems; however, in some cases, the cause is unknown. The displacement of implants occurs intraoperatively or within a short period because of insufficient surgical technique or anatomical variances of the jaws and is more frequent in the maxilla. Indeed, placement of implants in the maxilla is often complicated because of the low density of the maxillary bone and the insufficient bone height due to progressive resorption of the alveolar ridge. In the mandible implant displacement is unusual. In fact, implant migration into the marrow space is a complication that has been reported few times in the literature.
The aim of this cases report was to describe the clinical characteristics of patients who have developed displacement of an implant into the mandibular corpus.
Materials and Methods
Case I
A 66 year-old woman was referred to the Department of Oral Surgery of the University of Chieti-Pescara, Italy by her doctor for extraction of two premolars in the right mandible and right sinus lift. Her health history was unremarkable. The patient presented at this facility complaining of recurrent infection, tenderness and swelling in the lower right first and second premolars. A clinical examination of the patient revealed a buccal swelling. A panoramic radiograph was taken. The tooth mobility was tested with mild tenderness to percussion (Figure. 1). A periodontal probe was used to examine the pocket depth, revealing a depth of greater than 6 mm on the buccal side. The radiograph showed that the lower right second and first premolars had periapical radiolucency and incomplete root canal treatment. After discussing the options with the patient, she agreed to have the teeth removed and after a healing period of 2 months, two implants (Bone System, Milano, Italy) were placed to replace the missing teeth. No problems were reported during the implant placement, but during the positioning of the cover screws, the mesial implant disappeared, and a diffuse hemorrhage was observed that filled the oral cavity.
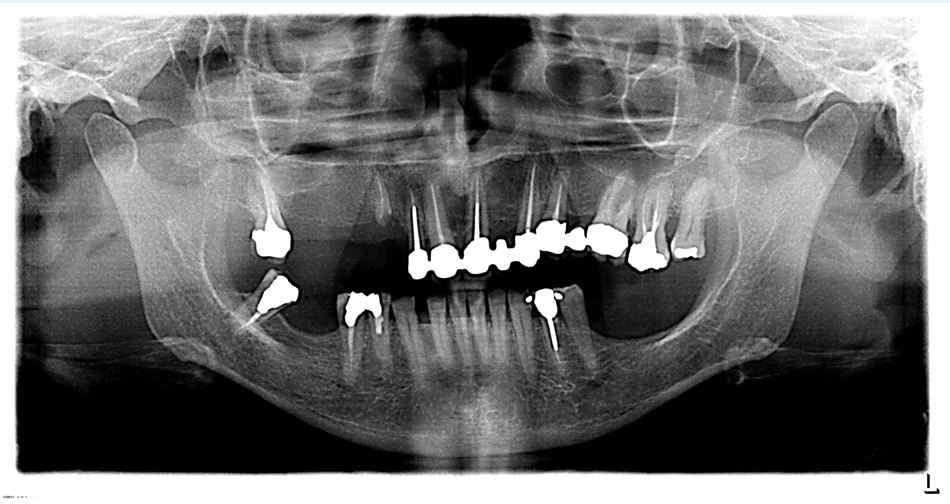
Figure 1: Preoperative panoramic radiograph that shows the edentulous ridges of the jaws. The fourth quadrant needs the placement of two dental implants in position 45 and 46, which one in a post extractive socket in the premolar area.
After clinical examination, a panoramic radiograph was taken. The radiograph showed the implant located near the mental nerve (Figure. 2). Before the implant was removed, a CBCT radiograph was taken of the exact location of the implant. The radiograph showed the implant in contact with the mandibular inferior border surrounded by a trabecular bone and laterally to the mental nerve (Figure. 3). The implant was removed by screwdrivers, the implant site was filled with a porcine bone xenograft (Tecnoss, Coazze, Turin, Italy) and the new implant was replaced immediately. Intraoral radiographs (baseline) were made with a paralleling technique to calculate the correct position for the implant. The patient was seen after 1 week for suture removal and after one month to evaluate together the surgical intervention.
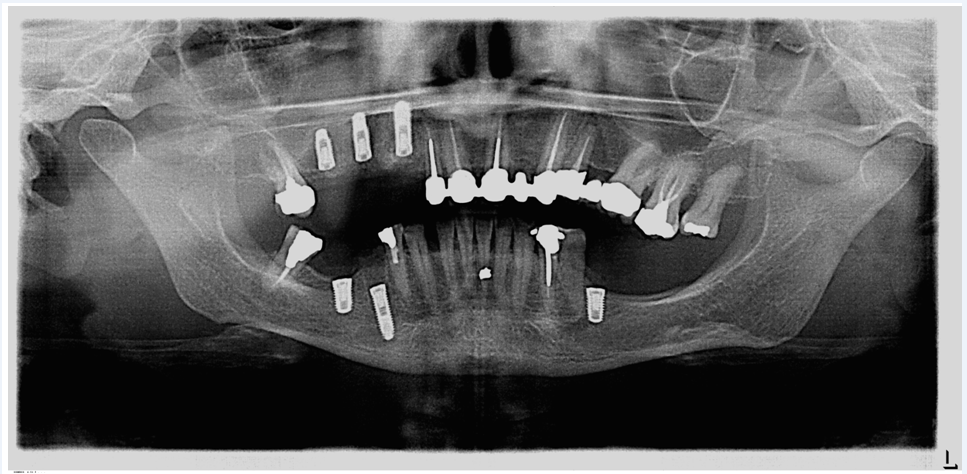
Figure 2: Immediate post-operative radiograph. The panoramic scanning shows an implant location near the mental nerve.
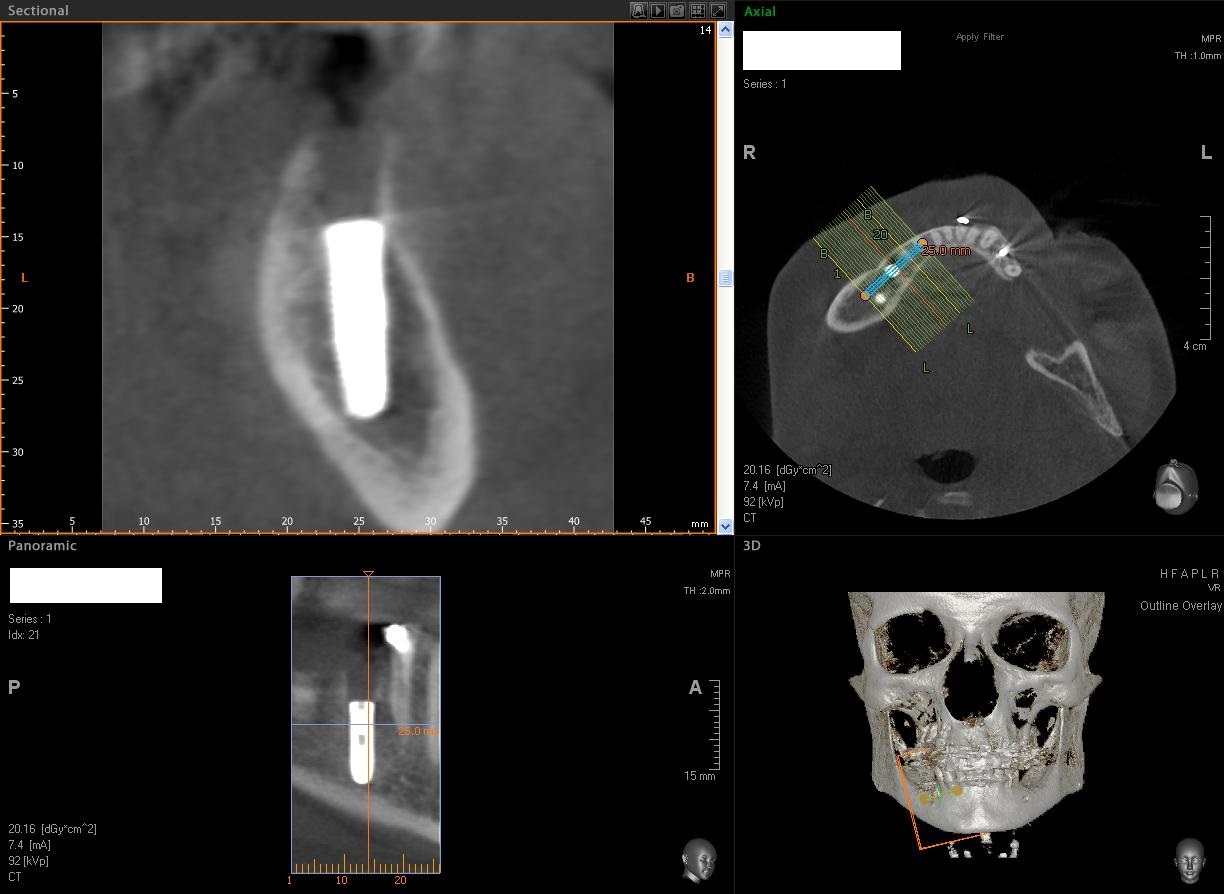
Figure 3: CBCT radiograph was taken to clarify the exact position of the fixture in the ridge. The scan shows the implant in contact with the mandibular inferior border surrounded by a trabecular bone and laterally on the mental nerve.
After 4 months of submerged healing (Figure. 4), the implant was exposed. The implant was manually tested for stability by loosening the cover screws. Within one-month, provisional screw-retained reinforced acrylic restoration, rigidly joining the implant, was delivered. Four months after delivery of the provisional prosthesis, definitive screw-retained metal-ceramic restoration rigidly joining the implant was delivered. At one week, the prostheses were checked, and the patient was given additional oral hygiene instructions.

Figure 4: Panoramic radiograph taken at 4 months from the surgery. After the submerged healing, the treated site showed a good osseointegration.
An X-Ray after 10 months showed a good integration. The patient received another implant in the left mandible without problem.
Case II
A 59-year-old woman was referred to the Department of Oral Surgery of the University of Chieti-Pescara, Italy by her dentist for implant placement in the left mandible molar. Her health history was negative for osteoporosis, irradiation treatment in the head and neck area, nor was she immunosuppressed or immunocompromised, nor had been treated or was under treatment with intravenous amino-bisphosphonates, for active periodontitis, poor oral hygiene and motivation, uncontrolled diabetes, nor pregnant or nursing, nor was she a substance abuser. Intraoral examination revealed healthy mucosa and there was no sign of infection. The panoramic radiograph showed a good height and the insertion of a 4 × 11 mm implant was programmed.
After discussing the options with the patient, she agreed to the placement of one implant (Implacil, De Bortoli, Sao Paulo, Brasil). No problems were reported during the implant bed preparation and placement but, also in this case, during the positioning of the cover screws the implant disappeared (Figure. 5). Taking the implant with a screwdriver was difficult because it was moving in the mandibular body. After trying to remove the implant with the screwdriver an osteotomy was performed with a Piezosurgery device (Mectron Piezosurgery Device™; Mectron S.p.a., Carasco Genoa, Italy), and the implant was removed with pliers. A bone graft (Tecnoss, Coazze, Turin, Italy) and collagen membrane (Tecnoss, Coazze, Turin, Italy) were used for filling the bone defect and a new implant was placed immediately. After 4 months of submerged healing the implant was exposed. The implants were manually tested for stability by loosening the cover screws. Within one-month, provisional screw-retained reinforced acrylic restorations, rigidly joining the implant were delivered. One month after delivery of the provisional prosthesis, definitive screw-retained metal-ceramic restoration rigidly joining the implant was delivered.
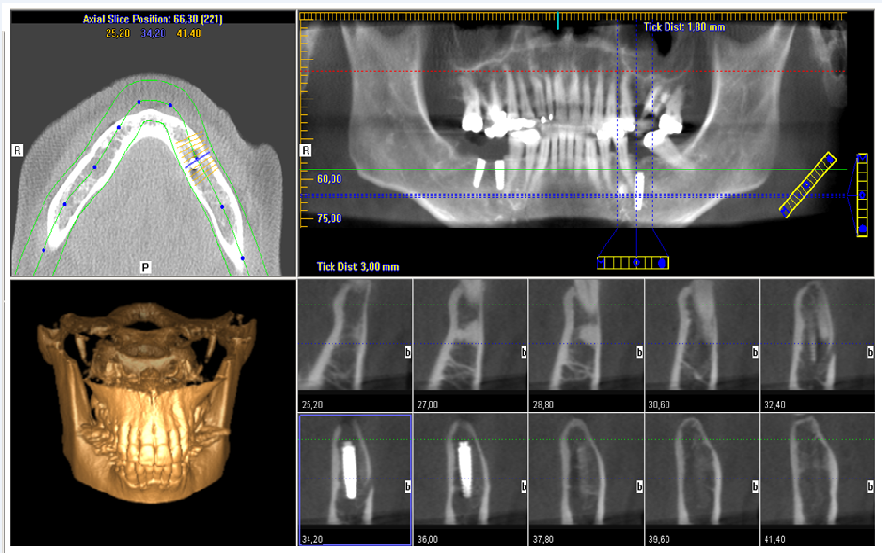
Figure 5: CBCT radiograph showing the implant in contact with the mandibular inferior border surrounded by a large medullary space and laterally on the mental nerve.
Case III
A 52-year-old man was sent to the Oral Surgery Clinic at the Department of Oral Surgery of the University of Chieti-Pescara, Italy for a first visit for a light pain in the left posterior mandible. Intraoral examination revealed a multiple implant placement with a complete rehabilitation with fixed prosthesis. After clinical examination, CBCT showed an implant displaced in the mandibular corpus and located in contact with the mandibular inferior border and laterally with the mental nerve (Figure 6). The coronal portion of the implant was 6 mm under the ridge and in the axis. Removal of the implant from the mandible depth was proposed. The patient refused to undergo this operation and remained asymptomatic for seven months after the migration of the implant. After 6 months the coronal portion of the implant was completely covered by new bone. The submerged healing implant was exposed after the healed bone had been removed with a Piezosurgery Device™ and a healing screw was applied on the coronal portion with many difficulties, but the coronal portion of the implant was not completely exposed. It was not possible to place an abutment at 6 mm under the ridge. After the difficulties of a provisional or definitive crown, the implant was removed by unscrewing and a new implant of 4 × 11 mm (Micerium S.p.A., Avegno, Genova, Italy) was immediately placed. After 4 months a healing screw was applied and the implant was stability.
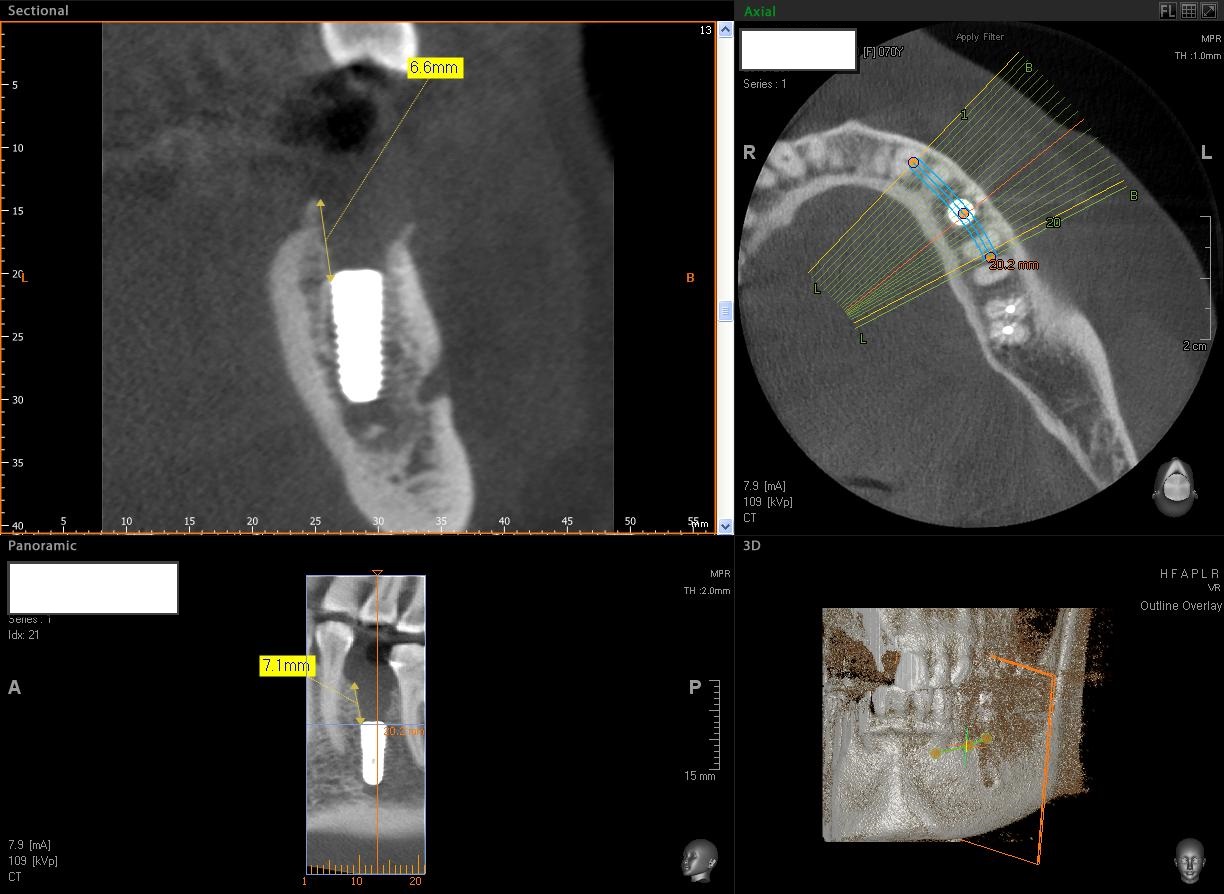
Figure 6: Multiplanar Reconstruction of CBCT scans. The implant appears displaced into the mandibular corpus; a large medullary space was present.
Discussion
In the present study, we report three cases of implants displaced into the mandible corpus. It is a rare complication in implantology; usually implant displacement in anatomical structures produces infection. For example, migration of an implant into the maxillary sinus is an uncommon finding, but this complication produces symptomatology, sinus inflammation and pain[5]. Here the displaced implant acts as a foreign body, producing chronic infection. Implants covered with debris will also act as foreign bodies and give rise to inflammation. Even more serious is the migration of implants into the sublingual space. The displacement of a foreign body into this anatomical space may provoke serious complications[6]. Pain, trismus, and swelling are present in the area and immediate root removal should be performed[8].
However, placement of endosseous implants in the posterior mandible has become a common procedure in recent years, although risks are still associated with the surgical or restorative therapy phase. It has been described that implants can be can be pushed into the sublingual space[8] but the migration of an implant into a mandibula corpus are unusual in clinical practice. The treated patients did not show radiological signs such as a large marrow space which observable with a panoramic radiograph, the CBCTs performed after the implant migration showed bone with a large trabecular bone and no other lesion or cyst was observed. All the implants were displaced laterally of the mental nerve. Probably in this area a bone with low density facilitates implant migration. The implant displaced in the mandibular bone do not produce inflammation or pain, but it is necessary to remove the implant for replacement with a new implant, also, the implants were localized laterally on the mental nerve without produce pain. Implant displacement into the mandibular corpus is not a serious complication but must be removed as soon as possible; otherwise the bone healing makes it difficult to remove them later. In one of the three cases we observed a sudden bleeding and a large amount of blood that filled the oral cavity. The mechanisms that explain the intraoperative and early displacement is low trabecular bone density, osteopenia or osteoporosis, and/or poor surgical technique, such as inadequate planning, overworking of the implant bed. Incorrect manipulation and mishandling have been suggested as possible factors[9]. The medullar component in the posterior mandible might be similar to that found in the maxilla and could facilitate the displacement of dental implants during surgery, probably caused by a focal osteoporotic bone marrow defect (FOBMD). This is a radiolucent area in edentulous areas of the jaws, most commonly seen in the posterior mandible of middle-aged women, corresponding to the presence of hematopoietic tissue rarely found in the jaws[10]. The exact cause of focal osteoporotic bone marrow defect is unknown but failure in bone repair in areas of trauma has been associated with its occurrence in edentulous regions where tooth extraction[10] or dental implant placement[10,12], such as in our case report, were previously performed. It is estimated that in most cases this lesion remains undetected. In all three cases the no radiolucent lesion in the premolar area was seen, but a trabecular bone was see by CBCT, while the panoramic radiograph did not show pathological lesion or trabecular bone. None of the patients had a medical history of osteoporosis. Recently, three cases of displacement of dental implants into the focal osteoporotic bone marrow defect have been documented by SC Lee et al.[13], the authors report that the final diagnoses of this condition were based only on clinical and radiographic findings. While Garcia et al.[12], described a case of a focal osteoporotic bone marrow defect associated with a dental implant which was diagnosed by histopathological analysis. They observed a hematopoietic marrow composed of monocytic, erythroid, granulocytic, and lymphocytic series as well as megakaryocytes associated with fatty marrow. In conclusion implant displaced into the mandible corpus is a rare complication, probably caused by a focal osteoporotic bone marrow defect (FOBMD) or a bone with a large and few trabecular, both are hardly identifiable by panoramic radiograph or CBCT.
Acknowledgements: The authors acknowledge the helpful technical assistance of Dr Mauro di Berardino (X-Ray Technician) in the elaboration of CBCT.
Disclosure: The authors claim to have no financial interest, either directly or indirectly, in the products or information listed in the paper.
References
1. Scarano, A., Carinci, F., Assenza, B., et al. Vertical ridge augmentation of atrophic posterior mandible using an inlay technique with a xenograft without miniscrews and miniplates: case series. (2011) Clin Oral Implants Res 22(10): 1125-1130.
2. Scarano A, Murmura G, Sinjiari B, et al. Expansion of the alveolar bone crest with ultrasonic surgery device: clinical study in mandible. (2011) Int J Immunopathol Pharmacol 24(2): 71-75.
3. Scarano A, Piattelli A, Murmura G, et al. Delayed expansion of the atrophic mandible by ultrasonic surgery: a clinical and histologic case series. (2015) Int J Oral Maxillofac Implants 30(1): 144-149.
4. Scarano, A., Sinjari, B., Murmura, G., et al. Neurosensory disturbance of the inferior alveolar nerve after 3025 implants placement. (2017) Implant Dent (Submitted) 26(5): 735-743.
5. Scarano, A., Perrotti, V., Carinci, F., et al. Removal of a migrated dental implant from the maxillary sinus after 7 years: a case report. (2011) Oral Maxillofac Surg 15(4): 239-243.
6. Aznar-Arasa, L., Figueiredo, R., Gay-Escoda, C. Iatrogenic displacement of lower third molar roots into the sublingual space: report of 6 cases. (2012) J Oral Maxillofac Surg 70(2): e107-115
7. Brauer, H.U. Unusual complications associated with third molar surgery: A systematic review. (2009) Quintessence Int 40(7): 565-572
8. Cariati, P., Fernández-Solís, J., Marín-Fernández, A.B., et al. Accidental displacement of a dental implant into the sublingual space: A Case report. (2016) J Clin Exp Dent 18(4): e459-461.
9. Theisen FC, Shultz RE, Elledge DA. Displacement of a root form implant into the mandibular canal. (1990) Oral Surg Oral Med Oral Pathol 70: 24-28.
Pubmed|| Crossref||Others
10. Sençimen, M., Delilbasi, C., Gülses, A., et al. Focal osteoporotic hematopoietic bone marrow defect formation around a dental implant: a case report. (2011) Int J Oral Maxillofac Implants 26: e1-4.
11. Makek, M., Lello, G.E. Focal osteoporotic bone marrow defects of the jaws. (1986) J Oral Maxillofac Surg 44(4): 268-273.
12. Garcia, N.G., Barros, F.B., Carvalho, M.M., et al. Focal osteoporotic bone marrow defect involving dental implant: a case report. (2015) Int J Implant Dent 1(1): 18-20.
13. Lee, S.C., Jeong, C.H., Im, H.Y., et al. Displacement of dental implants into the focal osteoporotic bone marrow defect: a report of three cases. (2013) J Korean Assoc Oral Maxillofac Surg 39(2): 94-99.










