
Non-compliance and its associated factors among hypertensive patients taking anti-hypertensive treatment visiting Gimbi general hospital,Western Ethiopia:cross-sectional study.
Firomsa Bekele1*, Dinka Dugassa2, Kumera Bekele3, Sanbato Tamiru4, Tigist Teklu5
Affiliation
1Department of Pharmacy, College of Health Science, Mettu University, Mettu, Ethiopia
2Nekemte referral hospital, Nekemte, Ethiopia
3Department of Nursing, College of Health Science, SelaleUniversity, Fiche, Ethiopia
4Department of nursing, College of Health Science, Mettu University, Mettu, Ethiopia
5Department of nursing, College of Health Science, Mettu University, Mettu, Ethiopia
Corresponding Author
Firomsa Bekele, Department of Pharmacy, College of Health Sciences Mettu University, Mettu, Ethiopia, Tel: +251(0)919536460; E-mail: firomsabekele21@gmail.com
Citation
Bekele, F., et al. Non-Compliance and its Associated Factors among Hypertensive Patients taking Anti-Hypertensive Treatment Visiting Gimbi General Hospital, Western Ethiopia: Cross-Sectional Study. (2019) J pharma pharmaceutics 6(2):65-71.
Copy rights
© 2019 Bekele, F. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Hypertension; Hypertensive treatment; Adherence; Compliance
Abstract
Background: Hypertension is defined as a persistent systolic Blood Pressure (BP) reading (SBP) of 140 mm Hg or greater and / or a Diastolic Blood Pressure Reading (DBP) of 90 mm Hg or greater and is an overwhelming global challenge which ranks third as a cause of disability-adjusted life-year. Poor adherence to anti-hypertensive therapy is one of the biggest obstacles in therapeutic control of high blood pressure and usually associated with bad outcome of the disease and wastage of limited health care resources. Control blood pressure can reduce cardiovascular morbidity and mortality, so the compliance and life style modification play an important role for the control of hypertension.
Objective: To assess the patient compliance and associated factors anti-hypertensive treatments in hypertensive patients visiting Gimbi general hospital.
Method: A hospital based cross-sectional study was conducted to all adult patients who visit medical OPD of Gimbi general hospital from March 5 to April 5 in 2018.
Result: The study showed that the overall level of compliance was 106 (83.46%) and non-compliance level was 21 (16.54%). Among 127 respondents 52 (40.94%) were males and 75 (59.06%) were females, 60 (47.24%) respondents had an income of 3.4-27.2 USD and 25 (19.7%) were employed. Majority of respondents 113(88.98%) were taking treatments as prescribed and 106 (83.36%) had regular follow up. In this study 45 patients never forget to take their medication and 82 (64 57%) respondents were stopped their medication due to different reason from this, 64 (34.8%) were due to improvement from illness and 37 (20.1%) due to lack of money.
Conclusion: The study showed that there was high compliance to antihypertensive treatment.
Improvements of the illness, prolong duration of treatment and Lack of enough money or income were the major factor that makes patients with HTN non-compliant with prescribed treatment regimes. Therefore, health professionals must educate the patient about disease with specific emphasis cause, severity of disease, their medication and consequences of non-adherence with treatment and the policy of sharing should be on the possibilities of giving antihypertensive drug free of charges.
Introduction
Hypertension is defined as a persistent systolic blood pressure (BP) reading (SBP) of 140 mm Hg or greater and / or a diastolic blood pressure reading (DBP) of 90 mm Hg or greater and is an overwhelming global challenge which ranks third as a cause of disability-adjusted life-year. It causes 7.1 million premature deaths each year worldwide and accounts for 13% of all deaths globally[1,2].
Analysis of the global burden of hypertension revealed that over 26% of the world’s adult population had hypertension in 2000[3]. In developing countries, its morbidity and mortality are increasing from time to time due to a change in life style and sedentary life. In Africa, 15% of the population has hypertension[4]. Although there is shortage of extensive data, 6% of the Ethiopian population has been estimated to have HTN. Approximately 30% of adults in Addis Ababa have hypertension above 140 / 90 mmHg or reported use of anti-hypertensive medication[5].
Medication compliance has been defined in terms of an agreement between the patient’s behavior of taking medications and the clinical prescription. Faulty compliance or non-compliance with medications may include errors of purpose, timing or dosage as well as total or partial omission, or use of inadvertent combinations. Non-compliance with medications is one of the major factors in the failure of therapeutic programs in patients having a chronic disease. In the available literature, the magnitude of non-compliance with medications prescribed for patients with hypertension was 16.7%[6,7].
The compliance of patient’s decreases with time and it is lower in long-term medications than in short-term medications. In depressive patients, compliance was shown to be 68% after 3 weeks of treatment, but this percentage decreased after 6, 9 and 12 weeks to 63%, 50% and 40% respectively . A compliance study conducted with short-term medications revealed an overall incidence of non-compliance of 26%. Ensuring patients’ compliance with anti-hypertension medications and lifestyle modifications to prevent complications of hypertension remains a major challenge to public health in many developing countries[8,9].
Non-compliance with treatment is the most important single reason for uncontrolled hypertension. Several factors, which may be patient or health system related, continue to militate against compliance behaviour. Thus it is essential to identify such factors and development strategies to improve compliance. It is true that the possible factors of non-compliance may vary from country to country and may contribute to the variations that exist among the reported values of non-compliance. With regard to the possible factors of non-compliance that are related to the patient, the disease, the drugs prescribed, the physician and the treatment environment ,the magnitude of non-compliance is expected to be high in Ethiopia, particularly study area[10,11].
Hypertension has no cure therefore; patients are expected to take medications for life. Drug treatments of hypertension demands that patients comply with their medications as prescribed and they should return for a refill when medications are exhausted. They should honor their appointments for follow up visits with clinician and adopt health actions that are recommended to lower their blood pressure[12]. Compliance with pharmacological and non-pharmacological treatment of hypertension has various benefits for the individuals, the health care systems and the society at large in the case of cost saving since it reduces the incidence of complications and the need for additional medications[13]. This is particularly crucial in a public financed health care system such as Ethiopia.
There are effective medical therapies for hypertension management. However, only 37% of hypertensive patients in a 2003-2004 survey were reported to have their blood pressure controlled[14].
The problem of non-adherence to medical treatment remains a challenge for the medical professions and social scientists. As a result, substantial numbers of patients do not get the maximum benefit of medical treatment, resulting in poor health outcomes, lower quality of life and increased health care costs. In spite of many advances made in adherence research, non-adherence rates have remained nearly unchanged in the last decades[7,15,16].
Poor adherence to anti-hypertensive therapy is one of the biggest obstacles in therapeutic control of high blood pressure. It also compromises the efforts of the health care system, policy makers and health care professionals in improving the health of populations. Failure to adhere causes medical and psychological complications of the disease, wastes health care resources and erodes public confidence in health systems[16,17].
In line with the global realities, Hypertension sufferers’ noncompliance to their pharmacological regimen and frequent lifestyle changes result in uncontrolled hypertension that leads to different life threatening organ complications such as cardiovascular, renal and cerebro-vascular diseases[18].
Concerning Client compliance towards antihypertensive treatment, specific studies are almost not exists in Gimbi. Little has been documented about the adherence status and associated factors in Ethiopia. Considering that HTN is a difficult disease for adherence to treatment due to the required change lifestyle habits and active participation of the individual in antihypertensive medication therapy[19]. Therefore, the main aim of this study was to add the existing body of knowledge about factors affecting compliance to hypertension medication and lifestyle modifications necessary to maintain hypertension control, and to propose strategies that will assist policy makers and clinicians with hypertension management decisions.
Methodology
Study setting and study period: A hospital based cross sectional study was conducted at GGH from March 5, to April 5, 2018. The Hospital was established and started its full function in 2005 and has different departments and wards like Outpatient department (OPD), medical ward, gynecology and obstetrics ward, pediatrics ward and surgical ward. It delivers diversified health services and clinics including the emergency services, eye clinic, dental clinic, mother and child health (MCH), laboratory, X-ray, and follow up of chronic disease. The Hospital possesses outpatient, inpatient, and ART pharmacies.
Study participants and eligibility criteria: All hypertensive people who were attending medical OPD during the study period and patients who agreed to participate in the study were included. People who are unable to give response for an informed consent, Patients less than 15 years of age, critically ill patients and mentally ill or psychiatric patients were excluded.
Study variables
Independent variables: Socio-demographic characteristics, such as: Age, Sex, Occupational status, Educational status, Religion, Ethnicity, Income, Marital Status, Area of residence, distance from their home to hospital.
Dependent variables: Prevalence of Non-compliance towards antihypertensive treatment
Prevalence of Non-compliance to lifestyle modifying service
Data collection process and management: Data was collected using questionnaire which was developed after reviewing different literature. The questionnaires were interviewed those all volunteer hypertensive people who fulfill the inclusion criteria while they was at medical OPD in GGH. The respondents were encouraged to answer the questions within the time they devoted as much as possible. And the data was collected through daily follow up.At each health unit selected interviewees was identified who fulfill the criteria while they exit after they get service. Every effort was made to choose a site for interviewing that allow the interviewer to be seat out of sight and at a sufficient distance from the health institute to avoid interviews being over heard each other. Five percent of the sample was pre-tested to check acceptability and consistency of data collection tool two weeks before the actual data collection.
Data processing and analysis: The data was entered in to computer using EPI-manager 4.0.2 software. Data checking and cleaning was done by principal investigator on daily basis during collection before actual analysis. Analysis was done using statistical software for social sciences (SPSS) 24. Descriptive data was generated and placed in terms of frequency and percentage. Descriptive statistics was used to analyze data in terms of frequency and percentage.
Operational definitions
Compliance: Is defined as “the extent to which a person’s behavior (taking medicines or executing lifestyle changes) coincides with medical or health advice” those taking medication daily[20,21].
Non-compliance: Any form of deviation from compliance like losing one appointment, missing doses, etc.(instructions not understood, costy, not availability of drug.)
Adherence: As “the extent to which a person behaviour taking medication following diet and or executing corresponds with agreed recommendations from health care provider.”
Concordance: Is patients have relationship with health care professionals and discuss with treatment and about the drug openly.
Hypertension: Is defined as the persistent systolic blood pressure equal to and greater than 140 mmHg and/or persistent diastolic blood pressure equal to and greater than 90 mmHg[13].
Hypertensive patient: Refers to a person diagnosed with hypertension as defined above
Results
Socio-demographic characteristics
A total of 127 study participants were interviewed making the response rate 100%. Most of the respondents were in the age range of 50-64 which make 54 (42.51%) of the respondents. Majority of the respondents 75 (59.06%) were females. Protestant Christians and the Gimbi towns hypertensive patients accounted for 70 (55.1%) and 54 (42.51%) of the respondents respectively. 54 (42.51%) of the respondents were rural by resident. About 73 (57.5%) of the patients were married and 48 (37%) of patients were illiterate and for 82 (64.57%) of the patients, it takes half an hour and above to reach the hospital.
Table 1: Socio demographic characteristic of the respondents in GGH, Oromia, western Ethiopia, from March 5 to April 5, 2018
|
Variables |
Frequency |
Percentage |
|
|
Sex |
Male |
52 |
40.94 % |
|
Female |
75 |
59.06 % |
|
|
Total |
127 |
100 % |
|
|
Age |
15-24 |
2 |
1.57 % |
|
25-49 |
46 |
36.22 % |
|
|
50-64 |
54 |
42.52 % |
|
|
>64 |
25 |
19.70 % |
|
|
Total |
127 |
100 % |
|
|
Religion |
Protestant |
70 |
55.10 % |
|
Orthodox |
33 |
26 % |
|
|
Muslim |
13 |
10.24 % |
|
|
Adventist |
11 |
8.66 % |
|
|
Total |
127 |
100 % |
|
|
Ethnicity |
Oromo |
121 |
95.20 % |
|
Amhara |
6 |
4.73 % |
|
|
Total |
127 |
100 % |
|
|
Educational status |
Illiterate |
48 |
37 % |
|
Read and write only |
9 |
7.08 % |
|
|
Primary |
37 |
29.15 % |
|
|
Secondary |
10 |
7.90 % |
|
|
College and above |
23 |
18.11 % |
|
|
Total |
127 |
100 % |
|
|
Occupations |
House wife |
18 |
14.17 % |
|
Farmer |
21 |
16.54 % |
|
|
Employment |
58 |
45.67 % |
|
|
Daily labor |
7 |
5.51 % |
|
|
Merchant |
14 |
11.02 % |
|
|
Others |
9 |
7.10 % |
|
|
Total |
127 |
100 % |
|
|
Marital status |
Married |
73 |
57.50 % |
|
Single |
25 |
11.80 % |
|
|
Divorced |
7 |
5.51 % |
|
|
Widowed |
32 |
25.20 % |
|
|
Total |
127 |
100 % |
|
|
Place of residence |
Urban |
73 |
57.49 % |
|
Rural |
54 |
42.51 % |
|
|
Total |
127 |
100 % |
|
|
Hours walk from Home to hospital |
<1/2 hr |
43 |
33.86 % |
|
1/2-1 hr |
22 |
17.32 % |
|
|
1-2 hrs |
34 |
26.79 % |
|
|
>2 hrs |
26 |
20.47 % |
|
|
Unknown |
2 |
1.57 % |
|
|
Total |
127 |
100 % |
|
|
Monthly income |
<3.4 |
31 |
24.42 % |
|
3.4-27.2 |
60 |
47.24 % |
|
|
27.2-40.8 |
11 |
8.66 % |
|
|
>40.8 |
25 |
19.68 % |
|
|
Total |
127 |
100 % |
|
Others includes Student and Nongovernmental organization
Compliance characteristics of patients to anti-hypertension treatments: Majority 113 (88.98%) of respondents, were taking treatment drugs as prescribed by health workers are compliant while only 14 (11.02%) were not taking as prescribed are not compliant.
Regarding the awareness towards treatments all (100%) respondents think that proper adherence to the prescribed treatments is important for improvement of disease; but only 118 (92.9%) of them are adherent to the prescribed treatment properly. All non-adherent 9 (7.1%) respondents namely of the participants responded that the rules of treatment compliance are difficult to fulfill as a reason for non-adherence.
Honoring clinic follow up appointment was considered to be a variable indicative of medication compliance. From the respondents more than three fourth had 106 (83.46%) have regular follow up while 21 (16.54%) do not have. Among participants who have regular follow up more than half or 67 (63.2%) have 1 months appointment while 36 (33.96%) have 1-3 month and only 3 (2.83%) respondents have appointment for more than 3 months. 101 (79.52%) were took their medication once per day, so more compliant, 21 (16.54%) were took twice per day and 5 (3.94%) were took three times per day so, less compliant.
Nearly two third of the respondents 94 (74.01%) have been on anti-hypertension treatments for more than a year duration. The others were 16 (12.6%) for 5-12 months, 13 (10.24%) for 2-5 months and 4 (3.15%) for less than 2 months (Table 2).
Table 2: Magnitude of follow up, treatment duration and frequency respondents to Anti-hypertension treatments, GGH, Oromia, Western Ethiopia, from March 5 to April 5, 2018
|
Variables |
Frequency |
Percentage |
|
|
Regular follow up |
Yes |
106 |
83.46 % |
|
No |
21 |
16.54 % |
|
|
Total |
127 |
100 % |
|
|
Taking drugs as prescribed |
Yes |
113 |
88.98 % |
|
No |
14 |
11.02 % |
|
|
Total |
127 |
100 % |
|
|
Frequency of drug taken per day |
Once |
101 |
79.52 % |
|
Twice |
21 |
16.54 % |
|
|
Three times |
5 |
3.94 % |
|
|
Total |
127 |
100 % |
|
|
Durationsince treatment Started |
<2 month |
4 |
3.15 % |
|
2-5 months |
13 |
10.24 % |
|
|
5-12 months |
16 |
12.6 % |
|
|
>1year |
94 |
74.01 % |
|
|
Total |
127 |
100 % |
|
Compliance and lifestyle modification regimens
Regarding lifestyle modification behavior, majority 91 (71.65%) of respondents were non-compliant while only 36 (28.35%) are compliant to physical exercise. The mean patient’s compliance to the lifestyle modifications regimen was 89.86, ± 29.2
Among non-recommended lifestyle modifying behaviors, 44 (34.64%) were stopped taking contra indicated substances during follow up. Out of 83 who were taking contra indicated substances 10 (12%) are taking only salt, 24 (28.9%) taking both coffee and salt, 33 (39.76%) taking coffee only, 5 (6%) taking only animal fat, 4 (4.82%) are taking both animal fat and coffee and 6 (7.2%) are taking animal fat, coffee and salt. 1 (1.2%) due to other reasons
Out of 127 respondents 98 (77.17%) never take alcohol while 29 (22.83%) responded as they consume in the following frequencies; among consumers 14 (48.27%) take sometimes, 2 (6.9%) take always andonly13 (44.83%) take rarely. From Hundred twenty seven respondents 121 (95.3%) never smoked cigarette, and 6 (4.72%) smoked from whom all of them smoked sometimes, always, rarely 2 (33.33) for each respectively. From 127 participants 115 (90.55%) never chewing khat (Catha edulis) and 12 (9.45%) chew in different frequencies like 10 (83.33%) sometimes, 2 (16.67%) always; but none of them chewing khat rarely (Table 2).
Regarding to perception all respondents (100%) think change in lifestyle modifying regimens is important in the improvement of disease.
Table 3: Number of respondents on avoidance of non-recommended and recommended behaviors on the Compliance and non-compliance hypertensive people in GGH, Oromia, Western Ethiopia from March 5 to April 5, 2018
|
Factors related to HTN |
Frequency |
Percentage |
|
|
Chewing khat |
Yes |
12 |
9.45 |
|
No |
115 |
90.55 |
|
|
Smoking |
Yes |
6 |
4.7 |
|
No |
121 |
95.3 |
|
|
Drinking alcohol |
Yes |
29 |
22.83 |
|
No |
98 |
77.17 |
|
|
Have regular exercise |
Yes |
36 |
28.35 |
|
No |
91 |
71.65 |
|
|
Drinking coffee |
Yes |
67 |
52.75 |
|
No |
60 |
47.25 |
|
|
Consuming fat |
Yes |
15 |
11.8 |
|
No |
112 |
88.2 |
|
|
Using salt on your meal |
Yes |
87 |
68.5 |
|
No |
40 |
21.5 |
|
Factors associated with anti-hypertension treatments non- compliance
This study showed that among the respondents 45 (35.43%) never forget to take medication, so they were compliant to their medication. 82(64.57%) respondent that they knew stopped their regular follow up and their medication previously with different purposes. From them 37 (20.1%) were due to lack of money, from this Still most of patients complain this purpose, due to improvement of illness 64 (34.8%), 15 (8.15%) no visible improvement, 13 (7.01%) negligence, 17 (9.24%) forgetfulness & 38 (20.7%) prolonged duration of treatment (figure 1). Among these 43 (52.43%) have been stopped treatment for less than 1 months, 26 (31.7%) for 1-3 months and 13 (15.85%) for more than 3 months, 75(91.46%) of them were started and planning to restart treatment and also take their drug as regimens again and 7 (8.54%) they have no idea about follow up. From the below result one patient complain one or more than one reason for noncompliance
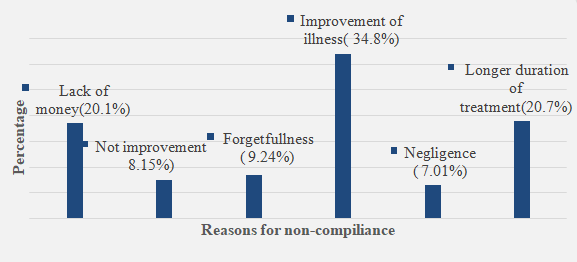
Figure 1: Reported reasons for non-compliance to anti-hypertensive treatments, GGH, Oromia, Western Ethiopia, from March 5 to April 5, 2018
Discussion
This study conducted to determine the levels of adherence and factors associated with non adherence to antihypertensive treatment and this study reveals that 83.46% were compliant. This was higher that the study conducted in Gondar 64.6%[22], Malaysia 44.2%[23], Gambia 27%[24], Egypt 74.1%[16] and lower than study done in Scotland 91%[25].
The study conducted in Seychelles and Dessie showed that the magnitude of adherence with anti-hypertension medications were 71.57% and 74% respectively[26,27] which was lower than our study.
The variation that existed among the literature value and with this study may partly be explained by the differences in the methods employed, economical status and educational advancement and may be different definitions of compliance and therefore; straight forward comparison and interpretation of the results may be difficult. In our study the level of compliance was lesser than the study done in Scotland. This might be because they are economically advanced to get needed drugs at time as well as more awareness than our countries people.
In the case of African countries all listed above reported lesser results than this study result. This might be the fact that the subjects of this study regularly visited the General hospital got instructions from their health care providers contributed their non-compliance behaviour
Non-compliant behaviour is dependent upon different interacting variables that are related to patients, illness and patients’ environment. Compliance with life modifications and avoidance of non-recommended behaviors’ are necessary to control blood pressure. A single study done in Yirgalem hospital, Southern Ethiopia on chronic illnesses showed that compliance magnitude of anti-hypertension regimens in adult population was 40% and lack of money was the major factor associated with treatment compliance which accounted 83% among other factors[28].
Here in this study also showed that the factors listed above were reported non-compliance with anti-hypertension treatments and lifestyle modification regimens. Longer distance was a big barrier for non-compliance to treatment recommendations especially when it was accompanied by poor infrastructure (e.g. lack of transportation) and poverty. This finding is supported by the study done in India[29]. Patients who take long time to come to the clinic have certain characteristics that promote non-adherence, which also delayed them from coming for review and possibly collecting drugs from the hospital when they refill the anti-hypertensive. Lack of money was reported as a limiting factor of patient compliance in this study. This is due to the fact that ant-hypertensive drugs were given for life long and provided by money in our study area.
The patients’ compliance to anti-hypertension treatments were urban people were more likely compliant than rural; this is may be information gap and accessibility of health facilities. Those who had high income were more likely compliant than those who low income. This might be happened because of they have enough money to buy treatment drugs. Patients who have been on treatment follow up for more than 12 months were more likely compliant than those who have been for 12 months and less. This is because patients may be familiar with treatment regimens and developed compliance behaviour through time.
Conclusion
The magnitude of adherence among hypertensive patients found to be higher. Patient’s attitude towards the medications they take was appreciable; the most influential factor to non-adherence was lack of money or income, negligence and improvement of illness and longer duration of treatment. The risk behaviours which were identified are insufficient physical exercise and insufficiently complied with the dietary requirements of limiting their consumption of animal fat, coffee, salt, alcohol, and smoking cessation.
In order to increase the magnitude of compliance to the medication health professionals must educate the patient about disease with specific emphasis cause, severity of disease, their medication and consequences of non-adherence with treatment and patients should be council led every time whenever they visit to improve the compliance to antihypertensive drugs. Additionally, government should be ensured adequate supply of antihypertensive drugs the policy of sharing should be on the possibilities of giving antihypertensive drug free of charges.
Acknowledgement
We thank Wollega University for funding this study. We are grateful to staff members and health care professionals of GGH, data collectors and study participants for their cooperation in the success of this study.
Authors’ Contributions
FB contributes in the proposal preparation, study design and analysis.GF contributed to the design of the study, analysis and write up of the manuscripts. DD and KB made a substantial contribution to the local implementation of the study. All authors read and approved the final version of the manuscript.
Ethics Approval and Consent-to-Participate
Ethical clearance was obtained from the ethics review board of Wollega University. Permission was obtained from medical director of the GGH to access hypertensive patients and conducts the study. The benefit and risks of the study was explained to each participant included in the study and written consent were obtained from each patient involved in the study. To ensure confidentiality, name and other identifiers of patients and health care professionals were not recorded on the data collection tools.
Consent for publication
Not applicable. No individual person’s personal details, images or videos are being used in this study.
Funding
The study was funded by Wollega University. The funder had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Availability of data and materials
The datasets used and / or analyzed during the current study are available from the corresponding author on reasonable request.
Competing Interests
No competing interests exist.
References
- Kearney, P.M., Whelton, M., Reynolds, K., et al. Global burden of hypertension:analysis of world wide data. (2005) Lancet 365(9455): 217-223.
- Chobanian, A.V., Bakris, G.L., Black, H.R., et al. Seventh report oftheJoint National Committee on Prevention, Detection, Evaluation, and Treatmen of High Blood Pressure. (2003) Hypertension 42(6): 1206-1252.
- Hajjar, I., Kotchen, T. A. Trendsinprevalence, awareness, treatment, and control of hypertensionin the United States, 1988–2000. (2003) JAMA 290(2): 199-206.
- Salako, L. A. Hypertension in Africa and Effectiveness of Its Management with Various Classes of Antihypertensive Drugs and in Different Socio-Economic and Cultural Environnements. (1993) Clin Exp Hypertens 15 (6) : 997-1004.
Pubmed| Crossref| Others
- Tesfaye, F., Byass, P., Wall, S. Population based prevalence of high blood pressure among adults in Addis Ababa:un covering a silent epidemic. (2009) BMC Cardiovascular Disord 9: 39.
- Sackett, D. L. The magnitude of compliance and non-compliance. (1976) Johns Hopkins University Press Baltimore: 9-25.
Pubmed| Crossref| Others
- Contreras, E.M., Main, C.G., etal. Observancia terapeutica enla hypertension arterial. (1995) Atencion Primaria 16(8): 496-500.
Pubmed| Crossref| Others
- Myers, E.D., Branthwaite, A. Out-patient compliance with antidepressant medications. (1992) Br J Psychiatry 160: 83-86.
- Abula, T. Patient non-compliance with therapeutic regimens and factors of non-compliance in Gondar. (2000) Ethiopia J Health Dev 14(1): 1-6.
- Benet, L.Z. Priciples of prescription order writing and patient compliance instructions, The pharmacological basis of therapeutics. (1996) INC NewYork: 1697-1706.
Pubmed| Crossref| Others
- Griffith, S. A review of the factors associated with patient compliance and the taking of prescribed medicines. (1990) Br J General Pract 40(332): 114-116.
- Greeff, D. An approach to preventing and treating hypertension through; Lifestyle modification. (2006) Professional Nursing Today 10(5): 8-22.
Pubmed| Crossref| Others
- Adherence to long-term therapies: evidence for action. (2003) World Health Organization.
Pubmed| Crossref| Others
- Ong, K.L., Cheung, B.M., Man, Y.B., et al. Prevalence, Awareness, Treatment, and Control of Hypertension Among United States Adults 1999–2004. (2006) Hypertension 49(1): 69-75.
- Primatesta, p., poulter, N.R. Improvement in hypertension management in England: results from health survey for England 2003. (2006) J Hypertension 24(6): 1187-119.
- Hashmi, S.K., Afridi, M.B., Abbas, K., et al. Factors associated with adherence to anti hypertensive treatment in Pakistan. (2007) PLoS One 2(3): e280.
- Balkrishnan, R. The importance of medication adherence in improving chronic-disease related outcomes: what we know and what we need to further know. (2005) Med Care 43(6): 517-552.
- Psaty, B. M., Lumley, T., Furberg, C.D., et al. Healthout comes associated with various antihypertensive therapies used as first-line agents: a network meta- analysis. (2003) JAMA 28(19): 2534-2344.
- Márcia, S. D., Edivan, R. de P. R., Eliane, R. P. Factors associated with adherence to antihypertensive treatment in primary care unit. (2012) Acta Paul Enferm 25: 27-34.
Pubmed| Crossref| Others
- Kaveh, L., Kimmol, P.L. Compliance in haemodialysis patients; multidimensional measures in search of Gold Standard. . (2001) Am J kidney Dis 37(2): 244-266.
- Bloom, B.S. Daily regimen & compliance with treatment. (2001) BMJ 323(7314): 647.
- Abere, D.A., Getahun, A. A., Solomon, M.W., et al. Adherence to Antihypertensive treatments and associated factors among patients on follow up at University of Gondar Hospital, Northwest Ethiopia. (2012) BMC public Health 12: 282.
- Morisky, D.E., Green, L.W., Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. (1986) MedCare 24(1): 67-74.
- van der Sande, M.A., Milligan, P.J., Nyan, O.A., et al. Blood pressure patterns and Cardiovascular risk factors in rural and urban Gambian communities. (2000) J Hum Hypertens 14(8): 489- 496.
Pubmed| Crossref| Others
- Rm, Y., II, M. Patterns and determinants of treatment compliance among hypertensive patients. (2002) East Mediterr Health J 8(4–5): 579-592.
- Thomas, A.E. Master of public health, University of south Africa, ,Factors affecting compliance with antihypertensive drug treatment and require lifestyle modifications among hypertensive patients on Praslin Island ,Seychelles (2009): 108-114.
Pubmed| Crossref| Others
- Chelkeba, L., Dessie, S. Antihypertension medication adherence and associated factors at Dessie hospital,North East Ethiopia. (2013) Int J Res Med Sci:1(3)
Pubmed| Crossref| Others
- Alexander, T., Enguday,S. Haregwoin, A., et al. Compliance and Factors related to treatment of chronic illness in adult population visiting Yirgalem Hospital (2006): 13-14.
Pubmed| Crossref| Others
- Inkster, M.E., Donnan, P.T., MacDonald, T.M., et al. Adherenceto antihypertensive medication and association with patient and practice factors. (2006) Hum Hypertens, 20(4): 295-297.










