
Prospective Review of Early Psychosis Following Traumatic Brain Injury in a Tertiary Hospital in Suburban Community of South Western Nigeria
Abiodun Idowu Okunlola1*, Cecilia Kehinde Okunlola2, Olakunle Fatai Babalola1, Tesleem Olayinka Orewole3, Chijioke Cosmas Achebe4
Affiliation
1Department of Surgery, Federal Teaching Hospital, Ido-Ekiti /Afe Babalola University, Ado-Ekiti, Nigeria
2Department of Medicine, Federal Teaching Hospital, Ido-Ekiti, Nigeria
3Department of Anaesthesia, Federal Teaching Hospital, Ido-Ekiti/Afe Babalola University, Ado-Ekiti, Nigeria
4Department of Radiology, Federal Teaching Hospital, Ido-Ekiti/Afe Babalola University, Ado-Ekiti, Nigeria
Corresponding Author
Dr. Abiodun Idowu Okunlola, Department of Surgery, Federal Teaching Hospital, Ido-Ekiti/ College of Medicine and Health Sciences, Afe Babalola University, Ado-Ekiti, Nigeria, Tel: +2348038112012; Email: okunlolab@yahoo.com
Citation
Okunlola, A.I., et al. Prospective Review of Early Psychosis Following Traumatic Brain Injury in a Tertiary Hospital in Suburban Community of South Western Nigeria. (2020) Int J Neuro Brain Dis 7(1): 4-6.
Copy rights
© 2020 Okunlola, A.I. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Psychosis; Traumatic brain injury; Antipsychotic medications; Propofol
Abstract
Background: The onset of psychotic symptoms after traumatic brain injury varies significantly in the literature with early onset psychosis most likely to present to neurosurgeons.
Aim: To document our experience with early posttraumatic brain injury psychosis
Methodology: Prospective review of patients who presented to our neurosurgical unit with psychotic symptoms following traumatic brain injury over a period of eighteen months from July 2018 to December 2019. Clinical and radiological profiles of the patients were documented prospectively.
Results: Five patients out of 145 patients (3.4%) with traumatic brain injury had posttraumatic brain injury psychosis using the Diagnostic and Statistical Manual for Mental Disorders 5th Edition. The onset of symptoms ranges between 7 to 17 days. There were three maleretired primary school teachers and two female students. Age ranges between 10 to 67 years. One patient had bilateral frontal burrhole drainage of the subdural hygroma under local anesthesia and sedation with propofol. There was complete resolution of the psychotic symptoms in the immediate postoperative period but these re-emerged about two hours post operatively.
Conclusions: Early onset psychosis following traumatic brain injury most likely will present to neurosurgeon and it responds to antipsychotic medications. Propofol may have a promising role in the management of post traumatic brain injury psychosis. There is need for long term follow up to evaluate the risk of recurrent psychosis.
Introduction
Psychosis is a rare devastating complication of head injury. The incidence ranges from 0.7% to 9.8% among the survivors of head injury[1]. The onset of psychotic symptoms after traumatic brain injury varies significantly in the literature with early onset psychosis most likely to present to neurosurgeons. It can occur as early as 2 days or delayed for several years[2,3]. Injury to the frontal and temporal lobes has been implicated as a risk factor in both closed and open head injuries[3,4]. It is more common in males than their females counterparts[3,5]. The diagnosis is mainly clinical and it must be distinguished from other mental disorders like schizophrenia. Diagnostic criteria have been established to aid prompt and appropriate diagnosis as follows; 1) presence of hallucination or delusion, 2) evidence that the psychosis is a direct consequence of traumatic brain injury, 3) psychosis is not better accounted for by another mental disorder and 4) psychosis does not occur exclusively during a state of delusion[6]. Psychosis following traumatic brain injury is an organic psychosis which usually responds to antipsychotic medications[3,7,8].
Aim: To document our experience with early post traumatic brain injury psychosis
Methodology: Prospective review of patients who presented to our neurosurgical unit with psychotic symptoms following traumatic brain injury over a period of eighteen months from July 2018 to December 2019. Clinical and radiological profiles of the patients were documented prospectively. The patients were followed up on the ward, and surgical outpatient clinic after discharge.
Results: We managed 145 patients for traumatic brain injury over 18 months and five (3.4%) patients had posttraumatic brain injury psychosis using the Diagnostic and Statistical Manual for Mental Disorders 5th Edition. The onset of symptoms ranges between 7 to 17 days. There were three male retired primary school teachers and two female students (table 1). Age ranges between 10 to 67 years (table 1). All were extroverts without family history of psychosis. Four patients were managed for mild traumatic brain injury with transient loss of consciousness at the time of trauma and one patient was managed for moderate head injury. There was no history of seizures, family or personal mental disorders, or alcohol use. Cranial CT scan showed bilateral subdural hygroma in the 3 male patients while the female patient had diffuse brain swelling. No other significant brain lesion.
Table 1: Patients’ profile
|
Age in years |
Sex |
Occupation |
Severity of head injury |
Aetiology |
Cranial CT scan findings |
Day of onset of psychosis |
Psychotic symptoms |
Medication |
Surgery |
|
65 |
Male |
Retired teacher |
Mild |
Pedestrian Motor Vehicular Accident |
Bilateral subdural hygroma |
7 |
Grandiose delusion, paranomia, disinhibition, hyperverbal speech |
Haloperidol |
nil |
|
65 |
Male |
Retired teacher |
Mild |
Rider Motorcycle Accident |
Bilateral subdural hygroma |
10 |
Persecutory delusion, paranomiadisinhibition, hyperverbal speech |
Haloperidol |
Bilateral frontal burrholedranage |
|
67 |
Male |
Retired teacher |
Mild |
Pedestrian Motorcycle Accident |
Bilateral subdural hygroma |
15 |
Paramnesia, wandering and picking trash |
Haloperidol |
nil |
|
26 |
Female |
Undergraduate student |
Mild |
Passenger Motorcycle Accident |
Brain swelling |
14 |
Paramnesia, wandering and picking trash |
Haloperidol |
nil |
|
10 |
Female |
Student |
Moderate |
Pedestrian Motor Vehicular Accident |
Diffuse brain swelling with punctate multifocal contusions |
17 |
Paramnesia, hyperverbal speech |
risperidone |
nil |
One patient had bilateral frontal burrhole drainage of the subdural hygroma (Figure 1: Cranial CT scan showing bilateral subdural hygroma) under sedation with a bolus of 1% intravenous propofol 5mls (50mg) and scalp infiltration with 10mls of 1% xylocaine with adrenaline. There was complete resolution of the psychotic symptoms in immediate postoperative period which recurred about 2 hours later. All patients were managed with antipsychotic medications with satisfactory response and they were weaned off the antipsychotic drugs within 2 months.
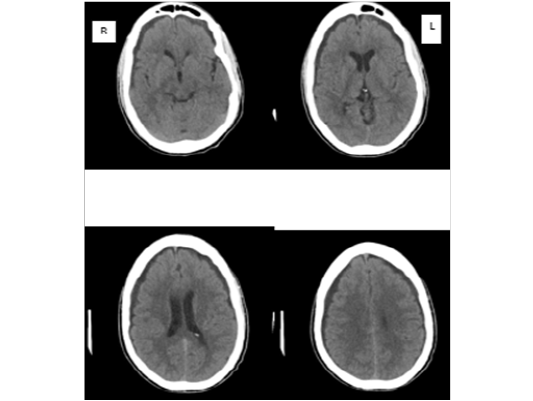
Figure 1: Cranial CT scan showing bilateral subdural hygroma
Discussion
Psychosis is a well-known complication of traumatic brain injury and it can occur irrespective of the severity of the initial head injury[4,9,10]. The relationship between head injury and neuropsychiatric manifestations is complex since majority of the affected patients present with psychosis years after the initial head injury, when the injury might have been forgotten[14,6,8]. Early presentation within 3 months of the initial head injury in a patient without prior history of behavioural psychiatric history is highly indicative of the head injury as an aetiological factor[9]. We reviewed clinical details of five patients who developed psychosis within a month of initial head injury which seems to have resolved until when the patient started psychiatric manifestations.
All five patients fulfilled the criteria for psychosis secondary to traumatic brain injury and had satisfactory response to antipsychotic medication. Previous reviews have linked head injury secondary to diffuse brain injury to neuropsychiatric manifestation similar to our experience in the index review[4,9]. Post-traumatic brain injury psychosis is common in male patients with traumatic brain injury than their female counterpart which may be as a result of the fact that the incidence of neurotrauma is higher in male than female[2,3,5,11].
Onset of symptoms varies significantly from a day to several years and schizophrenia has been attributed to childhood or birth trauma[2]. The very late psychotic manifestation in a patient with traumatic brain injury, though the incidence is higher than in general population, there are both genetic and environmental influences adduced but these are difficult to prove[12-14]. Early psychosis following head injury may clearly confirm traumatic head injury as a strong aetiological factor for development of neuropsychiatric disorders. There may be other factors which influence the onset of symptoms[9]. The psychosis following traumatic brain injury is a devastating complication which is distressing not only to the immediate relations of the patient but also to the society at large because behavioural anomalies as manifestation of the psychosis are highly stigmatized and have significant risk to both the patient and the society[8]. It significantly impact the quality of life of the individual patient[14]. Psychosis as a major challenge of the survivors of traumatic brain injury present a very strong point for primary prevention of head injury in the society[2,15].
The role of propofol in the management of psychosis is not yet explored. We incidentally noticed transient but complete resolution of the psychotic symptom in one of the patient who had borehole drainage of the bilateral subdural hygroma. The complete resolution of the psychotic manifestation was surprising but it recurred when the effect of the propofol disappeared. Richard Chalwin reported a case illustrating the superiority of propofol over the combined antipsychotic and sedatives in the transfer of a patient with acute psychosis[16]. This should stimulate more researches on the role of this agent in the management of neuropsychiatric disorders. The early psychosis following traumatic brain injury respond to antipsychotic medications but there is need for long term follow up to ascertain the risk of late recurrence.
Conclusion
Early onset psychosis following traumatic brain injury most likely will present to the neurosurgeon and it responds to antipsychotic medications. Propofol may have a promising role in the management of post traumatic brain injury psychosis. There is need for long term follow up to evaluate the risk of recurrent psychosis.
References
- 1. Rao, V., Lyketsos, C. Neuropsychiatric Sequelae of Traumatic Brain Injury. (2000) Psychosomatics 41(2): 95–103.
- 2. Fujii, D.E., Ahmed, I. Risk Factors in Psychosis Secondary to Traumatic Brain Injury. (2001) J Neuropsychiatry Clin Neurosci 13(1): 61–69.
- 3. Fujii, D., Fujii, D.C. Psychotic Disorder Due to Traumatic Brain Injury : Analysis of Case Studies in the Literature. (2012) J Neuropsychiatry Clin Neurosci 24(3): 278–289.
- 4. Chaudhury, S., Pande, V., Saini, R., et al. Neuropsychiatric Sequelae of Head Injury. (2005) Indian J Neurotrauma 2(1):13–21.
PubMed│CrossRef│Others
- 5. Nuhu, F.T., Yusuf, A.J. Psychiatric sequelae of traumatic brain injury : Retrospective analysis of 75 subjects from Kaduna, Nigeria. (2012) Niger J Clin Pract 15(4): 397–399.
- 6. David, A.S., Prince, M. Psychosis following head injury: A critical review. (2005) J Neurol Neurosurg Psychiatry 76(Suppl I): i53–i60.
- 7. Cittolin-santos, G.F., Fredeen, J.C., Cotes, R.O. Case Report A Case Report of Mania and Psychosis Five Months after Traumatic Brain Injury Successfully Treated Using Olanzapine. (2017) Case Rep Psychiatry 2017: 7541307.
- 8. Schwarzbold, M., Diaz, A., Hohl, A., et al. Psychiatric disorders and traumatic brain injury. (2008) Neuropsychiatr Dis Treat 4(4): 797–816.
- 9. Rao, V., Syeda, A., Roy, D., et al. Neuropsychiatric aspects of concussion : acute and chronic sequelae. (2017) Concussion 2(1): CNC29
- 10. Chaudhury, S., Biswas, P.S., Kumar, S. Psychiatric sequelae of traumatic brain injury. (2013) Med J Dr DY Patil Univ 6(3): 222–228.
- 11. Fujii, D., Ahmed, I. Characteristics of Psychotic Disorder Due to Traumatic Brain Injury : An Analysis of Case Studies in the Literature. (2002) 130 J Neuropsychiatry Clin Neurosci 14(2):130–140.
- 12. Tator, C.H., Davis, H.S., Dufort, P.A., et al. Postconcussion syndrome: demographics and predictors in 221 patients. (2016) J Neurosurg 125(5): 1206–1216.
- 13. Abdel Malik, P., Husted, J., Chow, E.W.C., et al. Childhood Head Injury and Expression of Schizophrenia in Multiply Affected Families. (2003) Arch Gen Psychiatry 60(3): 231–236.
- 14. Lathif, N., Phipps, E., Alton, P., et al. Prevalence of Psychiatric Disorders Following Brain Injury. (2014) Br J Med Pract 7(3): 7–9.
PubMed│CrossRef│Others
- 15. Kumar, R., Kumar, A., Kant, A. Psychosocial Impact of Brain Injury : A Review. (2019) Indian J Neurosurg 8: 11–15.
- 16. Chalwin, R. Propofol Infusion for the Retrieval of the Acutely Psychotic Patient. (2012) Air Med J 31(1): 33–35.










