
The Effect of Chewing Gum on the Pain Associated with Initial Placement of Fixed Orthodontic Appliances
Ajit Kalia, Ashwith Hegde and Kunal Mehta
Affiliation
Department of Orthodontics, M.A. Rangoonwala Dental College and Research Centre, Pune, Maharashtra, India.
Corresponding Author
Mueez Shedam, Department of Orthodontics, M.A. Rangoonwala Dental College and Research Centre, Pune, Maharashtra, India. Tel: 00918149507197; E-mail:moizshedam@gmail.com
Citation
Shedam, M. The Effect of Chewing Gum on the Pain Associated With Initial Placement of Fixed Orthodontic Appliances. (2015) J Dent & Oral Care 1(1): 1- 5.
Copy rights
© 2015 Shedam, M. This is an Open access article distributed under the terms of Creative Commons Attribution 4.0 International License.
Keywords
Fixed Orthodontic Appliances; chewing gum; Orthodontics
Abstract
Objectives: To determine the effect of chewing gum on the pain associated with initial placement of fixed orthodontic appliances.
Sample population: Subjects were selected from the Department of Orthodontics, who wanted to undergo fixed orthodontic therapy.
Subjects and Methods: A randomized clinical trial with two parallel groups allocated to receive chewing gum after initial placement of their appliance or who were asked not to use Chewing (chewing) gum. Subjects completed a compliance form and visual analogue scale (VAS) to assess the intensity of pain at 24hrs and after 1week following placement of the initial working archwire.
Results: Values are Median (Minimum– Maximum). P-value by Mann-Whitney U test (Un-paired analysis using non-parametric methodology). P-value < 0.05 is considered to be statistically significant.
1) 24-Hrs and 7-Days post treatment average pain scores differ significantly in Non-Chewing Study group (P-value < 0.001).
2)The average pain score after 24-Hrs is significantly higher in Non-Chewing Gum group (P-value < 0.001).
3) The average pain score after 7-Days is significantly higher in Non-Chewing Gum group compared to Chewing Gum group (P-value < 0.001).
4) The average change in pain score after 7-Days is significantly higher in Non-Chewing Gum group compared to Chewing Gum group (P-value < 0.001).
Conclusion: Chewing gum significantly decreased pain from the fixed appliances.
Introduction
It has been shown that fixed orthodontic appliances lead to a deterioration in both adolescent[1,2] and adult[3] oral health-related quality of life (OHRQoL), particularly in the first month after placement. This is related to the functional and social discomfort associated with wearing a fixed appliance[4], as well as the physical discomfort and pain[5,6]. This impact on OHRQoL may affect compliance and may lead to patients failing to complete treatment.
Research shows that 90% of orthodontic patients reported that their treatment was painful and 30% considered ceasing treatment prematurely because of the pain they experienced[7]. The commonest method of controlling the pain and discomfort from orthodontic appliances investigated has been the use of systemic analgesics[8].
The use of local pharmaceutical agents has also been investigated[9]. Non-pharmological methods include transcutaneous electrical nerve stimulation[10] and lasers[11]. Despite these research findings, there is no standard of care for analgesic use in the pain management of orthodontic patients. It is more common for orthodontists to simply tell their patients to take analgesics as needed, leaving pain management decisions up to their mostly adolescent patients and their parents[12,13].
Orthodontic appliances cause discomfort and can affect eating, speaking, smiling and other activities. Some patients give up treatment early because of the impact on their everyday life. We should therefore do all we can to minimize this impact[14]. One simple intervention is to advise patients to chew gum when it suits them. However, there are few clinical studies examining either the positive or negative effects in patients with fixed orthodontic appliances, which hopefully are addressed with this study. This study found that chewing gum reduced the impact and discomfort of fixed appliances without the negative effects of causing more breakages.
Materials and Methods
This study was a randomized trial, consisting of 60 randomly selected subjects undergoing orthodontic treatment in the Department of Orthodontics and Dentofacial Orthopaedics and were divided into 2 groups (30 patients each). Subjects were between the age of 13 and 30 years and those undergoing fixed orthodontic therapy, with all permanent dentition and habit of brushing twice daily with toothpaste and toothbrush were only included in the present study. Patients with use of anti-inflammatory or antibiotic medications taken in the month before the study and use of chewing gum or mouthwash used in the last week of the study were excluded. Also patients with habit of smoking/alcohol/tobacco and having pre-existing gum diseases were excluded.
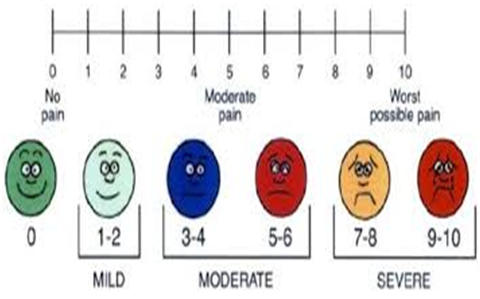
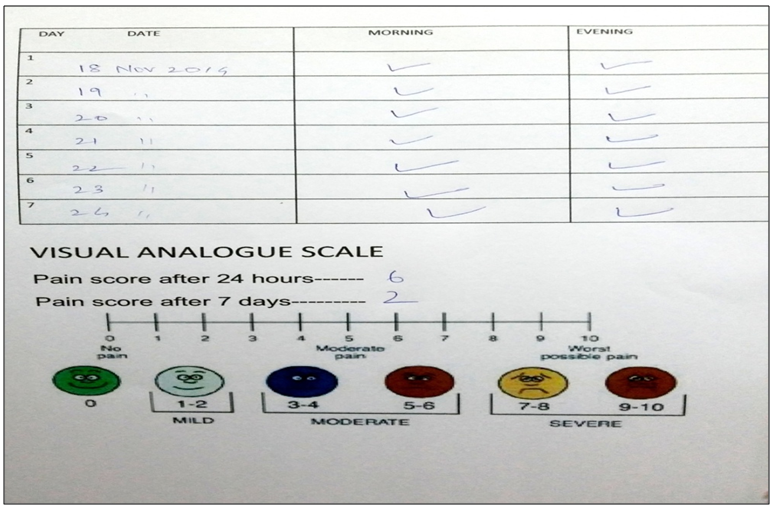
The patients in Group I were given sugar free chewing gum (Figure 1) to be chewed daily twice in morning and evening respectively for a period of one week[16,17]. The patients in group 2 were asked not to chew gum for a period of one week Patients were asked to fill up a compliance schedule daily for taking chewing gum. Compliance schedule form (Table 1) was handed to the patient before trial. Visual analogue scale (Figure 2) was given to both the group to be filled up at the fixed schedule of 24 hours and after one week. Patient were asked to mark appropriate score depending upon the degree of pain felt (Figure 3).

Table 1: Compliance schedule chart
| DAY DATE | MORNING | EVENING |
|---|---|---|
Results
Majority of subjects were in between fifteen to nineteen years in this study (Table 2, Figure 4). In the present study it was observed that sex distribution of the volunteers did not differ significantly between two study groups (P-value > 0.05) (Table 3, Figure 5). However, majority of volunteers were females across two study groups.
Table 2: Age distribution of the volunteers studied across two study groups. Values are n (% of volunteers). P-value by Chi-Square test. P-value < 0.05 is considered to be statistically significant. S: Statistically Significant, NS: Statistically Non-Significant.
| Age Group (Years) | Non-Chewing gum group (n = 30) Group (n = 30) | Chewing Gum Group(n = 30) | P-value |
|---|---|---|---|
| < 15.0 | 7 (23.4) | 5 (16.6) | 0.580 (NS) |
| 15.0 – 19.0 | 13 (43.3) | 17 (56.7) | |
| > = 20.0 | 10 (33.3) | 8 (26.7) | |
| Total | 30 (100.0) | 30 (100.0) |
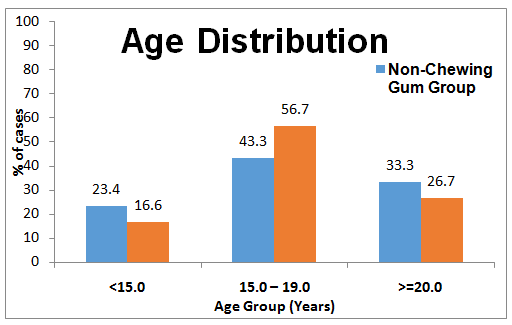
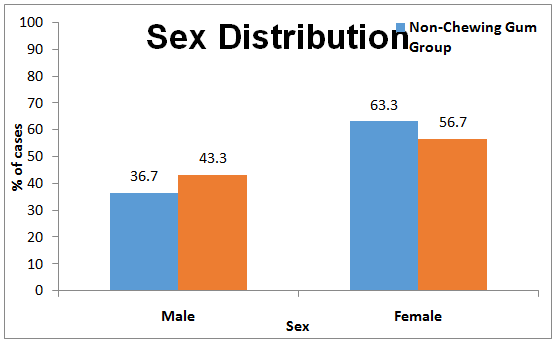
Table 3: Sex distribution of the volunteers studied across two study groups. Values are n (% of volunteers). P-value by Chi-Square test. P-value < 0.05 is considered to be statistically significant. S: Statistically Significant, NS: Statistically Non-Significant.
| Sex | Non-Chewing Gum Group (n=30) | Chewing Gum Group (n=30) | P-value |
|---|---|---|---|
| Male | 11 (36.7) | 13 (43.3) | 0.598 (NS) |
| Female | 19 (63.3) | 17 (56.7) | |
| Total | 30 (100.0) | 30 (100.0) |
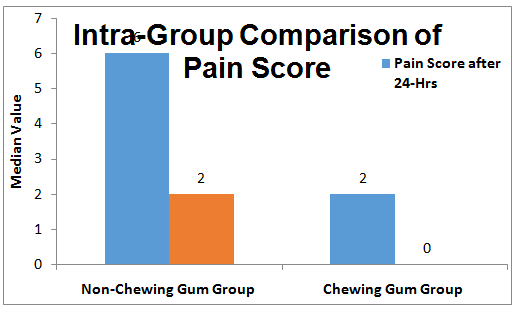
The average pain score after 24hrs was significantly higher in Non-Chewing Gum group compared to Chewing Gum group (P-value < 0.001).The average pain score after 7 Days was significantly higher in Non-Chewing Gum group compared to Chewing Gum group (P-value < 0.001).The average change in pain score after 7 Days was significantly higher in Non-Chewing Gum group compared to Chewing Gum group (P-value < 0.001) (Table 4, Figure 6).
Table 4: Intra-Group Comparison of Pain Score in each study groups. Values are Median (Minimum – Maximum). P-value by Wilcoxon's Signed Rank Test (Paired analysis using non-parametric ethodology). P-value < 0.05 is considered to be statistically significant. S: Statistically Significant,NS: Statistically Non-Significant.
| Pain Score | Non-Chewing Gum Group (n=30) | Chewing Gum Group (n=30) |
|---|---|---|
| Pain Score after 24-Hrs | 6 (3 – 8) | 2 (0 – 5) |
| Pain Score after 7-Days | 2 (0 – 3) | 0 (0 – 2) |
| P-value (After 24Hrs v After 7Days) | 0.001 (S) | 0.001 (S) |
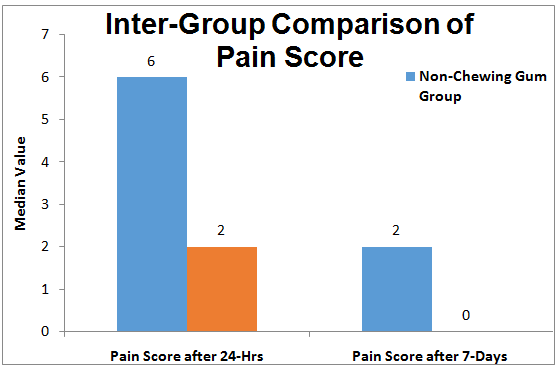
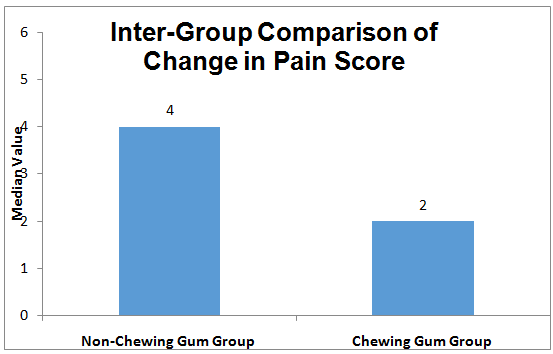
The change in pain score was significantly higher in chewing gum group as compared to non-chewing gum group (Table 5, Figure 7ab).
Table 5: Inter-Group Comparison of Pain Score in each study groups. Values are Median (Minimum – Maximum). P-value by Mann-Whitney U test (Un-paired analysis using non-parametric methodology). P-value < 0.05 is considered to be statistically significant. S: Statistically Significant, NS: Statistically Non-Significant.
| Pain Score | Non-Chewing Gum Group (n=30) | Chewing Gum Group (n=30) | P-value |
|---|---|---|---|
| Pain Score after 24-Hrs | 6 (3 – 8) | 2 (0 – 5) | 0.001 (S) |
| Pain Score after 7-Days | 2 (0 – 3) | 0 (0 – 2) | 0.001 (S) |
| Change in Pain Score | 4 (0 – 6) | 2 (0 – 5) | 0.001 (S) |
Discussion
Subjects were also asked to complete a compliance sheet twice which was given to them, they were specifically asked to fill up the time daily when they took chewing gum and to tick mark on compliance sheet handed over to them. We chose to use a single summary measure of impact and pain (the median score) at 24 hours and 1 week interval Generally, 24 h after fixed appliance placement adjustment is considered the peak time for pain, which then reduces over the next week[18,19]. Even though we have given compliance sheet to be filled by the patient, our limitation was few subjects did not took the chewing gum.
We found no significant differences between boys and girls for the median score. Subjects in chewing gum group said that the chewing gum helped relieve the pain and discomfort, some subjects said chewing gum distracted their attention from the pain and discomfort. Others found that chewing gum did not help when the teeth were painful.
We also found out that chewing gum helped to keep the appliance clean, and few patients said that sometimes the chewing gum does help release food that gets stuck in the braces.
The additional potential benefit of chewing gum increasing salivary flow and helping clean the appliance and possibly reduce demineralization would be an interesting topic for future studies.
Conclusion
Chewing gum significantly reduced the amount of pain from the fixed appliance after initial placement and activation as compared to subjects not taking chewing gum.
References
- 1. Bernabe, E., Sheiham, A., Tsakos, G., et al. The impact of orthodontic treatment on the quality of life in adolescents: a case control study. (2008) Eur J Orthod 30(5): 515- 520.
- 2. Zhang, M., McGrath, C., Hagg, U. Changes in oral health-related quality of life during fixedorthodontic appliance therapy. (2008) Am J OrthodDentofacialOrthop 133(1): 25- 29.
- 3. Liu, Z., McGrath, C., Hagg, U. Changes in oral health-related quality of life during fixed orthodontic appliance therapy: an 18-month prospective longitudinal study. (2011) Am J OrthodDentofacialOrthop 139(2): 214- 219.
- 4. Sergl, H. G., Klages, U., Zentner, A. Functional and social discomfort during orthodontic treatment–effects on compliance and prediction of patients adaptation by personality variables. (2000)Eur J Orthod 22(3): 307– 315.
- 5. Scheurer, P. A., Firestone, A. R., Burgin, W. B. Perception of pain as a result of orthodontic treatment with fixed appliances. (1996)Eur J Orthod 18(4): 349- 357.
- 6. Krukemeyer, A. M., Arruda, A. O., Inglehart, M. R. Pain and orthodontic treatment. (2009) Angle Orthod 79(6): 1175- 1181.
- 7. Otasevic, M., Naini, F. B., Gill, D.S., et al. Prospective randomized clinical trial comparing the effects of a masticatory bite wafer and avoidance of hard food on pain associated with initial orthodontic tooth movement. (2006) Am J Orthod Dentofacial Orthop 130(1): 6.e9- 6.e15.
- 8. Bradley, R. L., Ellis, P. E., Thomas, P., et al. A randomized clinical trial comparing the efficacy of ibuprofen and paracetamol in the control of orthodontic pain. (2007) Am J Orthod Dentofacial Orthop 132(4): 511- 517.
- 9. Kluemper, G. T., Hiser, D. G.,Rayens, M.K., et al. Efficacy of a wax containing benzocaine in the relief of oral mucosal pain caused by orthodontic appliances. (2002) Am J Orthod Dento facial Orthop 122(4): 359- 365.
- 10. Roth, P. M.,Thrash,W.J.Effect of transcutaenous electrical nerve stimulation for controlling pain associated with orthodontic tooth movement. (1986) Am J Orthod Dentofacial Orthop 90(2): 132- 138.
- 11. Turhani, D., Scheriau, M., Kapral, D., et al. Pain relief by single low-level laser irradiation in orthodontic patients undergoing fixed appliance therapy. (2006) Am J Orthod Dentofacial Orthop 130(3): 371- 377.
- 12. Polat, O.,Karaman,A. I., Durmus,E.Effects of Preoperative Ibuprofen and Naproxen Sodium on Orthodontic Pain. (2005) Angle Orthod 75(5): 791- 796.
- 13. Kemppainen, P.,Vaalamo, I., Leppa, N., et al. Changes in tooth pulpal detection and pain thresholds in relation to jaw movement in man. (2001)Arch Oral Biol 46(1): 33- 37.
- 14. Furstman, L., Bernick, S. Clinical considerations of the Periodontium. (1972) Am J Orthod 61(2): 138- 155.
- 15. Miller, K. B., McGorray, S. P., Womack, R., et al. A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment. (2007) Am J Orthod Dentofacial Orthop 131(3): 302.e1- e9.
- 16. Mandall, N.A., Vine, S., Hulland, R., et al. The impact of fixed orthodontic appliances on daily life. (2006) Community Dent Health 23(2): 69- 74.
- 17. Bernabe, E., Sheiham, A., de Oliveira, C. M. Impacts on daily performances related to wearing orthodontic appliances. (2008) Angle Orthod 78(3): 482– 486.
- 18. Bergius, M., Berggren, U., Kiliaridis, S. Experience of pain during an orthodontic procedure. (2002) Eur J Oral Sci 110(2): 92- 98.
- 19. Erdinc, A. M., Dincer, B. Perception of pain during orthodontic treatment with fixed appliances. (2004) Eur J Orthod 26(1): 79- 85.










